Proximal Nerve Conduction Studies in Upper Extremity and Cervical Plexus
Surface Anatomy and Brachial Plexus Stimulation at Erb’s Point
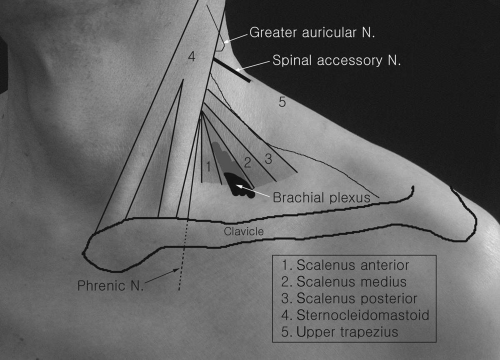 Figure 5-1. Anatomy of supraclavicular fossa and brachial plexus. |
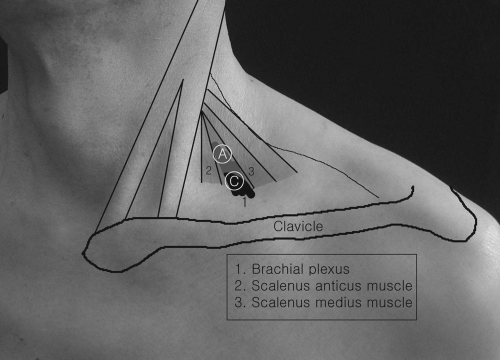 Figure 5-2. Brachial plexus stimulation point at the supraclavicular fossa/Erb’s point stimulation. |
The brachial plexus lies in the supraclavicular fossa, between the clavicle and the lower part of the posterior border of the sternocleidomastoid. It emerges between the scalenus anterior and scalenus medius. When the arm is by the side, the plexus can be felt as a bunch of tense cords with a relative firm press by a finger tip 2 to 3 centimeters (cm) proximal to the anterior convexity of the medial two-thirds of the clavicle. This area may match with Erb’s point, a point 2 or 3 cm above the clavicle and beyond the posterior border of the sternocleidomastoid, at the level of the transverse process of the sixth cervical vertebra. The stimulating cathode placed at this point can stimulate the brachial plexus. The patient’s head can be turned to the opposite side of stimulation. The stimulation site is identified when the patient notes discomfort with firm pressure over the plexus. Because the brachial plexus is crossed by many different structures (arterys, veins, muscles, and nerves other than plexus) at this point, supramaximal stimulation is often difficult to achieve, requiring high current intensities with a long duration of pulse. Stimulation at Erb’s point can stimulate the entire brachial plexus, not an individual nerve, so some degree of a volume-conducted muscle response from adjacent muscles may be inevitable.
Distance Measurement
Accurate measurement of distance between the stimulation and recording points in proximal motor conduction is often difficult and inaccurate. Measurements
with an obstetrical caliper is best, although a flexible tape can be used. Most previous tests were done with unfixed distances.
Axillary Nerve Conduction to the Deltoid
(Fig. 5-3)
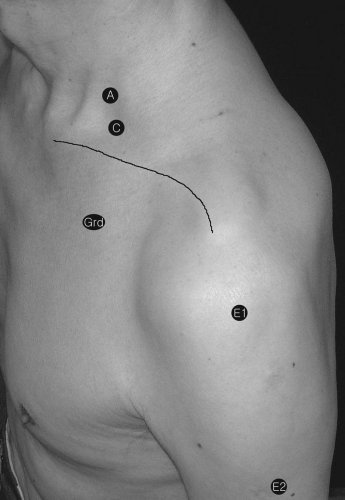 Figure 5-3. Axillary nerve conduction studies to the deltoid muscle. |
Recording Electrode Placements
Stimulation
The cathode is placed in the supraclavicular fossa, just lateral to the sternocleidomastoid muscle. The anode is positioned proximal to the cathode. Stimulation
applied at Erb’s point stimulates the brachial plexus (trunk—upper, middle, and lower). Firm pressure applied at Erb’s point and a long-pulse duration [˜1 milli- second (ms)] by the stimulator are often necessary to evoke an optimal compound muscle action potential (CMAP).
applied at Erb’s point stimulates the brachial plexus (trunk—upper, middle, and lower). Firm pressure applied at Erb’s point and a long-pulse duration [˜1 milli- second (ms)] by the stimulator are often necessary to evoke an optimal compound muscle action potential (CMAP).
Musculocutaneous Nerve Conduction to the Biceps Brachii
(Fig. 5-4)
 Figure 5-4. Musculocutaneous nerve conduction studies to the biceps brachii. |
Recording Electrode Placements
Stimulation
Supraclavicular fossa (see page 100 for details)
Suprascapular Nerve to the Supraspinatus and Infraspinatus Muscles
Supraspinatus Muscle Recording
A standard concentric needle is inserted medial to the midpoint of the scapular spine and just above the spine. It is directed in a downward and
anterior direction until bone contact is made, and then the needle is withdrawn slightly. Shoulder abduction may confirm the needle placement. The study is done with patients either sitting or side–lying with arms at the side.
Infraspinatus Muscle Recording
(Fig. 5-5)
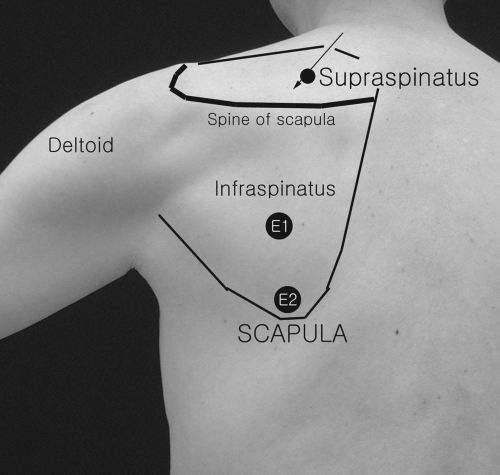 Figure 5-5. Suprascapular nerve conduction studies to the supraspinatus and infraspinatus muscles with Erb’s point stimulation. |
Surface or needle electrodes can be used. The surface E1 electrode is placed several centimeters lateral to the medial border of the scapula and 2 to 3 cm below the scapular spine. The E2 surface electrode is positioned 2 cm more distal to the stimulating cathode. Also, needle electrodes may be used as above noted.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


