 Posterolateral Approach to the Ankle
Posterolateral Approach to the AnkleThe posterolateral approach is used to treat conditions of the posterior aspect of the distal tibia and ankle joint. It is well suited for open reduction and internal fixation of posterior malleolar fractures. Because the patient is prone, however, it is not the approach of choice if the fibula and medial malleolus have to be fixed at the same time. In such cases, it is better to use either a posteromedial approach or a lateral approach to the fibula, and to approach the posterolateral corner of the tibia through the site of the fractured fibula. Neither of these approaches provides such good visualization of the bone as does the posterolateral approach to the ankle, but both allow other surgical procedures to be carried out without changing the position of the patient on the table halfway through the operation. Its other uses include the following:
Excision of sequestra
Removal of benign tumors
Arthrodesis of the posterior facet of the subtalar joint
Posterior capsulotomy and syndesmotomy of the ankle
Elongation of tendons
Position of the Patient
Place the patient prone on the operating table. As always, when the prone position is being used, longitudinal pads should be placed under the pelvis and chest so that the center portion of the chest and abdomen are free to move with respiration. A sandbag should be placed under the ankle so that it can be extended during the operation. Next, exsanguinate the limb by elevating it for 3 to 5 minutes or applying a soft rubber bandage; then inflate a tourniquet (Fig. 6-1).
Landmarks and Incision
Landmarks
The lateral malleolus is the subcutaneous distal end of the fibula.
The Achilles tendon is easily palpable as it approaches its insertion into the calcaneus.
Incision
Make a 10-cm longitudinal incision halfway between the posterior border of the lateral malleolus and the lateral border of the Achilles tendon. Begin the incision at the level of the tip of the fibula and extend it proximally (Fig. 6-2).
Internervous Plane
The internervous plane lies between the peroneus brevis muscle (which is supplied by the superficial peroneal nerve) and the flexor hallucis longus muscle (which is supplied by the tibial nerve; Fig. 6-3).
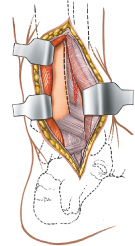
Superficial Surgical Dissection
Mobilize the skin flaps. The short saphenous vein and sural nerves run just behind the lateral malleolus; they should be well anterior to the incision. Incise the deep fascia of the leg in line with the skin incision, and identify the two peroneal tendons as they pass down the leg and around the back of the lateral malleolus (Fig. 6-4). The tendon of the peroneus brevis muscle is anterior to that of the peroneus longus muscle at the level of the ankle joint and, therefore, is closer to the lateral malleolus. Note that the peroneus brevis is muscular almost down to the ankle,
whereas the peroneus longus is tendinous in the distal third of the leg (see Figs. 26-1 and 26-2).
whereas the peroneus longus is tendinous in the distal third of the leg (see Figs. 26-1 and 26-2).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


