Plantar Fasciitis
Kristen Kuratnick
David I. Pedowitz
 A 46-year-old woman who is an avid runner presents complaining of gradual worsening of heel pain over course of 5 months. She notes most severe pain with the first steps out of bed in the morning and at the end of her shift as a waitress. The pain is localized to the medial aspect of her heel. |
CLINICAL PRESENTATION
The plantar fascia is a band of fibrous tissue extending from the plantar calcaneal tuberosity to the flexor tendon expansion in the forefoot. Its function is to support the longitudinal arch of the foot in what is called a “windlass mechanism.” Briefly explained, the windlass mechanism refers to the concept that as the toes are dorsiflexed, the plantar fascia is placed on stretch, thereby dynamically accentuating the longitudinal arch of the foot.
Plantar fasciitis is the most common cause of heel pain in the 40- to 60-year-old age group who often present with the insidious onset of heel pain. Start-up pain is a classic complaint with worse symptoms upon getting out of bed in the morning and at the end of a workday. Pain is typically nonradiating and abates with rest. Although the etiology is multifactorial, independent risk factors include obesity, work-related weight bearing, and decreased ankle dorsiflexion.1 Additionally, runners and athletes seem to be prone to plantar fasciitis likely as a result of repetitive microtrauma to the fascia.
CLINICAL POINTS
Most common cause of heel pain.
Morning start-up pain is a typical complaint.
Multifactorial etiology including running, obesity, prolonged standing, and decreased ankle dorsiflexion.
PHYSICAL FINDINGS
Physical exam should address both gait and stance. Gait is usually unaffected. During stance, exam may reveal a foot deformity such as pes planus or pes cavus. These deformities may increase load on the plantar fascia causing pain at the origin or along the length of the fascia. Point tenderness is noted at the origin of the plantar fascia on to the medial tubercle of the calcaneus. One must differentiate this finding from a positive squeeze test at the posterior body of the calcaneus, which in the setting of swelling may indicate a calcaneal stress fracture. Pain is often exacerbated when the toes are passively dorsiflexed placing the plantar fascia on stretch.2
Decreased ankle dorsiflexion on the affected side as compared to the unaffected foot suggests a tight gastrocsoleus complex. A thorough neurologic exam must be completed to rule out peripheral neuropathy from diabetes, radiculopathy, or nerve compression as the cause of heel pain. A plantar fascial rupture presents acutely with possible loss of the medial longitudinal arch and a palpable fascial defect. These patients often also relay a history of trauma, a pop that is felt in the arch, and significant plantar ecchymosis. Plantar fibromatosis is differentiated on exam by palpable nodules and pain at the midsubstance of the fascia. This is a benign entity and is typically treated with accommodative orthotics with recesses for the large nodules. Surgery is typically avoided due to the high recurrence rate and the irritating plantar incisions.3
STUDIES (LABS, X-RAYS)
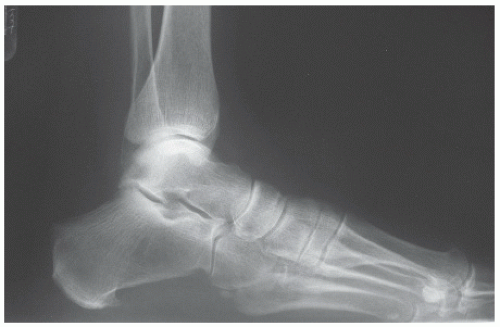
Weight-bearing radiographs of the foot are often of limited utility in the initial workup of plantar fasciitis. Unless the patient presents with atypical history (i.e., trauma) or unusual symptoms or exam findings, they should be obtained after several weeks of conservative treatment. A common, often incidental finding on lateral radiograph is a heel spur, once thought to play a role in plantar fasciitis (Fig. 28-1). It
is generally accepted that the heel spur seen on x-ray is not the source of pain, and simple removal is not the cure for this malady. The heel spur is located within the flexor digitorum brevis muscle origin—not the plantar fascia.
is generally accepted that the heel spur seen on x-ray is not the source of pain, and simple removal is not the cure for this malady. The heel spur is located within the flexor digitorum brevis muscle origin—not the plantar fascia.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


