Pediatric Ankle Fractures
Scott J. Mubarak
Andrew T. Pennock
DEFINITION
Ankle fractures account for about 5% of all pediatric fractures and are second only to distal radius fractures as the most prevalent physeal fracture comprising approximately 15% of these injuries.1
As in most pediatric trauma, nonoperative management is the mainstay of treatment; however, surgical indications can be specific to the pediatric population.
Much like adults, surgical treatment is indicated when there is any significant articular incongruity or angular deformity.
Classification of pediatric ankle fractures can be a practical tool for both the treatment and prognosis of these fractures.
The most common classification scheme for pediatric ankle fractures is the Salter-Harris method for physeal fractures.
The Lauge-Hansen classification used in adults can be modified for pediatric ankle fractures and aids in conceptualizing the reduction technique by reversing the fracture pattern. Also, previous studies have shown that pronation-type injuries have a higher rate of premature physeal closure than supination-external rotation (SER) type injuries.7
This classification is useful as most orthopaedic surgeons are familiar with it.
Transitional fractures of the ankle occur near skeletal maturity and are due to the asymmetric closure of the distal tibial physis.
Triplane fracture is described as a complex Salter-Harris type IV fracture that consists of sagittal, transverse, and coronal components with an epiphyseal and metaphyseal fragment.
Tillaux fractures occur most often in adolescents within 1 year of distal tibial physeal closure. They involve an external rotational force that avulses the anterolateral aspect of the tibial epiphysis, which is attached to the anterior inferior tibiofibular ligament, which is stronger than the residual open physis.
ANATOMY
The ligaments of the ankle attach to the epiphyses provide stability to the ankle mortise. These ligaments contribute to the pathomechanics of transitional fractures (triplane and Tillaux fractures) because they are often more stout than the growth plate, leading children to sustain physeal fractures more readily than ankle sprains.
The anteroinferior tibiofibular ligament attaches to the anterolateral border of the tibial epiphysis, and with an external rotation force on the foot, it has the ability to avulse the anterolateral fragment of the tibial epiphysis; the strength imbalance between the ligament and weaker physis can create the transitional Tillaux and triplane fractures.
The anatomy of the distal tibial physis is relevant to understanding certain ankle fractures and their management and prognosis.
The secondary ossific nucleus of the distal epiphysis appears between 6 and 24 months, with the apophysis of the medial malleolus often extending from an elongation from this ossific nucleus or from a separate ossification center, the os subtibiale, which ossifies between 7 and 8 years of age.
The distal tibial physis is primarily transverse; however, there is an anteromedial undulation that consistently appears within the first 2 years of life that has been described by Kump (termed Kump bump). This centromedial location is where physiologic physeal closure begins (FIG 1).
Physeal closure of the distal tibia occurs around 15 years of age in girls and 17 years of age in boys.
Closure progresses from the centromedial location of Kump bump medially, then laterally from this location, over about 18 months.
The anatomy of the physis also influences ankle fractures in children.
The perichondral ring of LaCroix is a transitional area between the articular cartilage and the periosteum of the diaphysis. Made of perichondrium, it retains the potential for producing cartilage and bone.
Functionally, the perichondral ring provides stability to the physis and may play a role in certain fractures and growth plate injuries in children.
Adjacent periosteum which rigidly attaches to the perichondral ring can become interposed in the fracture site and obstruct anatomic reduction.
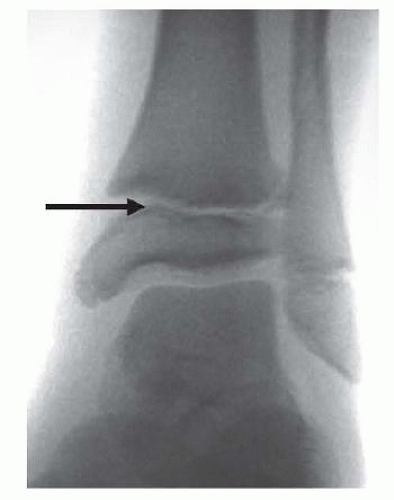 FIG 1 • Kump bump. The arrow demonstrates the centromedial-located Kump bump, which is where physeal closure begins. We believe that damage to this structure may induce premature physeal closure. |
PATHOGENESIS
The Lauge-Hansen classification system was developed in 1950 to understand the injury mechanism by reproducing fracture patterns in adult cadavers.4
This classification is a two-part classification, with the initial portion describing the position of the foot at the time of injury (eg, supination, pronation) and the following portion describing the direction of the deforming force, either rotational (internal or external) or translational (abduction or adduction).
This system grades the severity of ankle injuries as I to IV in rotational patterns and I to II in translational patterns.
A recent series of 114 classifiable ankle fractures (Salter II) using the Lauge-Hansen system, SER composed 66%; abduction, 30%; pronation-external rotation, 3%; and axial crush injuries, 1%.7
The activity that resulted in ankle fractures varied in our series, with most occurring during falls and sports.1, 7
SER fractures did not seem to have any specific activity that was more likely to produce premature physeal closure; however, abduction injuries occurring with soccer or skateboarding were much more likely to develop premature physeal closure when compared to other activities.
Specific anatomy and growth plate closure patterns create certain fractures in adolescence.
For example, the same external rotation mechanism can produce a Tillaux or a triplane fracture, depending on the age and degree of physeal closure of the child.
The lateral portion of the distal tibial physis closes last. This is often an area of weakness in the skeletally maturing child, allowing an anterolateral fragment to be avulsed from the epiphysis, creating Tillaux fractures or the intraarticular fragment in the triplane fracture.
NATURAL HISTORY
Premature physeal closure of the distal tibia has been historically described as a rare sequela in physeal fractures, with an incidence as low as 2% to 5%.1
Our recent data demonstrate an overall 38% incidence of physeal arrest in Salter-Harris I type and II fractures but maybe as high as 55% for displaced fractures. Both the mechanism of injury and and treatment modality have been shown to influence the rate of premature closure.7, 8
SER injuries have a better prognosis for premature physeal closure, with a 38% overall incidence, as compared to abduction-type injuries, with a 52% overall incidence.
This difference in prognosis between SER and abduction injuries may be explained by the shearing force of Kump bump that may occur in abduction injuries, as opposed to less traumatic rotational force to this anatomic structure that occurs with SER injuries.
These data have prognostic relevance in pediatric ankle fractures, as an earlier series demonstrated a 3.5-fold increase in the premature physeal closure rate if a gap of 3 mm or more was present on the postreduction imaging of Salter-Harris types I and II fractures.
Our experience suggests that periosteum interposed in the physis leads to residual fracture gapping and may contribute to premature physeal closure.
The orthopaedic surgeon should discuss the potential for premature physeal closure with the family at the initial visit, particularly with an abduction type of injury.
PATIENT HISTORY AND PHYSICAL FINDINGS
As in adult trauma, the initial evaluation of a child’s ankle injury consists of eliciting the mechanism and timing of injury.
Basic examination should consist of evaluating the skin and soft tissues, finding areas of maximal tenderness to palpation, and obtaining an accurate sensory, motor, and vascular examination.
Particular issues that must be considered in the diagnosis of ankle fractures in children include osteomyelitis and child abuse.
Osteomyelitis has a prevalence of 1 per 5000 children. It generally occurs in the vascular loops of the metaphyseal regions of bone in children and can occur because of hematogenous spread or as a result of trauma, which can further complicate diagnosis.
A thorough history of the proximity of pain onset relative to the inciting trauma will help differentiate trauma from infection.
Metaphyseal fractures of the distal tibia in children can be concerning for child abuse, as the mechanism can be attributed to forceful pulling or twisting of the extremity, fracturing the cancellous bone through the metaphysis. Additional concerns are bilateral extremity fractures and fractures at different stages of healing.
Visualization of the skin is critical in the evaluation for potential open injuries. The quality of skin can also affect the timing of surgical fixation and give insight into the energy and location of injury.
Palpation of the ankle can assist in locating the injury and may allow diagnosis of occult physeal fractures or ligamentous injuries not seen on radiographs.
Establishing preoperative deficits is critical in the pre- and postoperative management of ankle fractures and may aid in establishing the need to release the extensor retinaculum compartment.
Preoperative deficits can be due to nerve contusion or laceration, in addition to tendon disruption or mechanical block. This can affect the surgical approach.
Vascular status is the key to the ultimate viability of the extremity. If deficits are found, the fracture should be immediately reduced. If a deficit is still present after reduction, a vascular study may be considered versus immediate operative exploration to evaluate for transient spasm or vascular injury.
IMAGING AND OTHER DIAGNOSTIC STUDIES
If there is any suspicion of an ankle injury, a complete radiographic ankle series should be performed consisting of an anteroposterior (AP), a lateral, and a mortise view (FIG 2A-C).
The mortise view is critical and is taken from anterior to posterior with the foot internally rotated 20 degrees to view the talus with a symmetric clear space seen medially and laterally.
The importance of the mortise view is seen in Tillaux fractures, where the anterolateral fragment is often obscured by the overlap of the posterior fibula on the AP view and is not well visualized on the lateral view.
We do not advocate stress radiographs in children; however, we will use an external rotation stress view intraoperatively to evaluate for syndesmosis injury if suspected in children near skeletal maturity.
Accessory ossicles can be commonly visualized on plain radiographs and may be confused with ankle fractures.
These include the os subtibiale medially (up to 20% of population), the os trigonum posteriorly (about 10% of population), and the os fibulare laterally (about 1% of population).
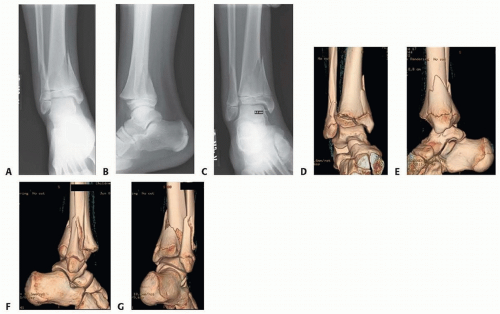
FIG 2 • Triplane fracture imaging. All ankle fractures require a plain radiographic series comprising AP (A), lateral (B), and mortise views (C). D-G. Three-dimensional CT reconstructions can aid in operative planning, especially for the difficult to visualize intra-articular fractures.
Contralateral comparison films may be helpful to differentiate accessory ossicles from a fracture.
Computed tomography (CT) is required to fully understand many ankle fractures, and we often advocate three-dimensional postreduction CT scans (FIG 2D-G).
We advocate CT scans for intra-articular fractures that show residual displacement on plain radiographs after attempted closed reduction.
At time of injury for Salter-Harris types I and II fractures and triplane fractures of the distal tibia, in addition to the standard radiographs, it can be helpful to obtain an AP view of the left hand to establish bone age and contralateral radiographs for a baseline physeal comparison.
DIFFERENTIAL DIAGNOSIS
Ankle sprain
Accessory ossicle
Osteochondral lesion (osteochondritis dissecans)
Contusion
Osteomyelitis
NONOPERATIVE MANAGEMENT
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


