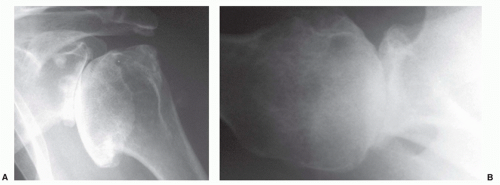
 FIGURE 12-1. (A) True anteroposterior view of the glenohumeral joint and (B) transaxillary lateral view, adequately demonstrating moderately severe osteoarthritis. |
relation of the humerus to the glenoid and acromion process, the width of the articular cartilage, osseous erosions, productive changes including osteophytes, and the presence of soft tissue swelling and calcification.
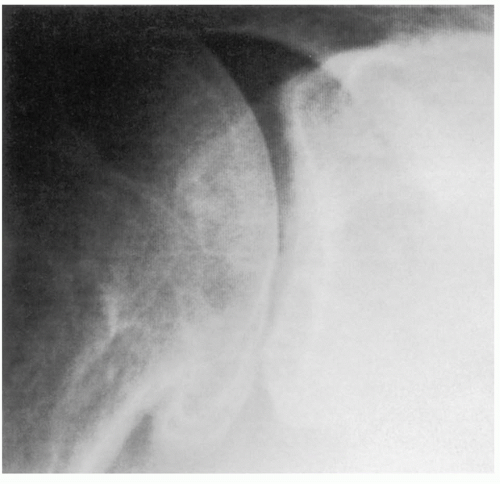 FIGURE 12-2. Humerus in 35 degrees of external rotation, profiling the articular surface in the true anteroposterior plane of the scapula. |
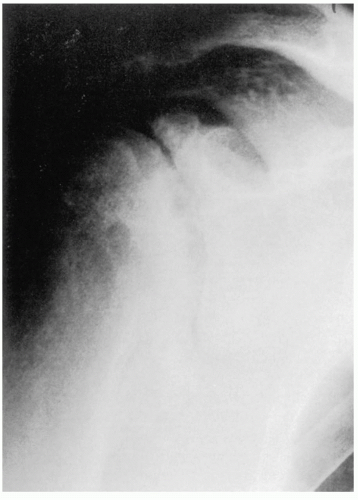 FIGURE 12-3. More advanced osteoarthritis, requiring total rotation of the humerus with the torso, a result of fixed internal rotation contracture of the glenohumeral joint. |
good spatial resolution for the detection of small defects, good subject contrast and image contrast for the detection of signal intensity changes in articular cartilage, reliable distinctions for the detection of signal intensity changes in articular cartilage, and reliable distinction between articular cartilage and adjacent subchondral bone and joint fluid.323 Broderick’s study drew attention to the tendency for cartilage abnormalities to be underestimated with MRI when compared with arthroscopic observations.77 Amin made a similar observation when MRI was compared with radiographic progression.17 The use of injectable contrast agents to enhance the detection accuracy of articular cartilage is not generally necessary.118,433,523
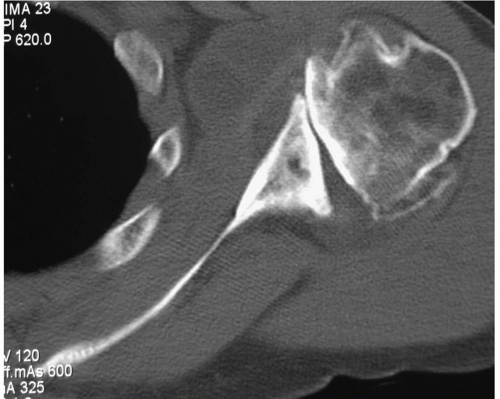 FIGURE 12-4. Computed tomography scan of osteoarthritis demonstrating a biconcave glenoid. There is posterior glenoid erosion that has a radius of curvature distinctly different from the anterior glenoid, where a small amount of articular cartilage persists. Peripheral humeral head osteophytes are apparent. |
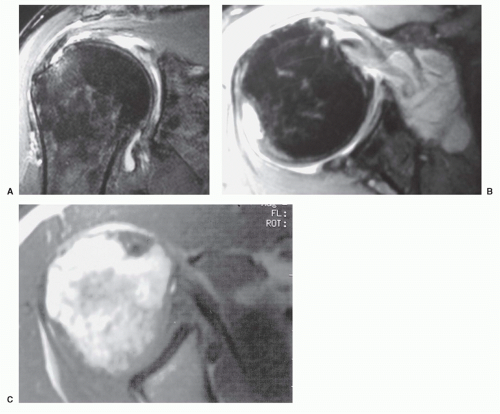 FIGURE 12-5. (A,B) Magnetic resonance imaging (MRI) demonstrating abnormal accumulation of joint fluid as well as osteoarticular changes commonly seen in glenohumeral osteoarthritis. (C) MRI with obliteration of the glenohumeral joint space by proliferating pigmented villonodular synovitis. |
Directed toward the coracoid process, the needle will penetrate the deltoid and infraspinatus muscles to enter through the capsule into the joint.
TABLE 12-1 Synovial Fluid Analysis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
observed in joint sepsis. Synovial fluid protein is often increased in inflammatory disease. The utility of synovial fluid glucose and protein levels is questionable.786 Appropriate organism stains and cultures should be obtained when there is even the most remote suspicion of an infectious process.
that has irreversibly changed load-response characteristics.559 Fragments of extracellular matrix proteins have been shown to bind to receptor sites on chondrocytes, inducing chondrolysis.652,680,878 As a result, the capacity for cartilage to repair appears to fail, a dysfunction that ultimately leads to its loss.
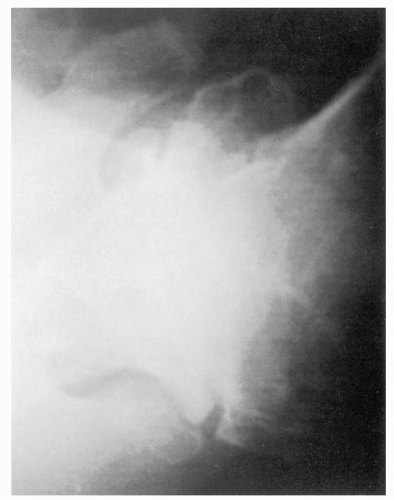 FIGURE 12-6. Osteoarthritis: Axillary lateral view with enlargement and flattening of the humeral head. There is concentric erosion of the glenoid. |
compressive forces were a prerequisite for the development of osteoarthritis.578 He further believed that an enlarged osteoarthritic head helps prevent upward migration, resulting in fewer impingement-type rotator cuff tears.578 Rupture of the biceps tendon long head can rarely occur, but the mechanism is in response to the presence of spurs in the intertubercular groove and not by the process of impingement against the coracoacromial arch.578 The subacromial bursa has been noted to be thickened in the absence of acromial pathology in a high percentage of patients.850 During the arthroscopic evaluation and treatment of glenohumeral arthritis, the incidence of a concomitant lesion requiring treatment was 47%.104
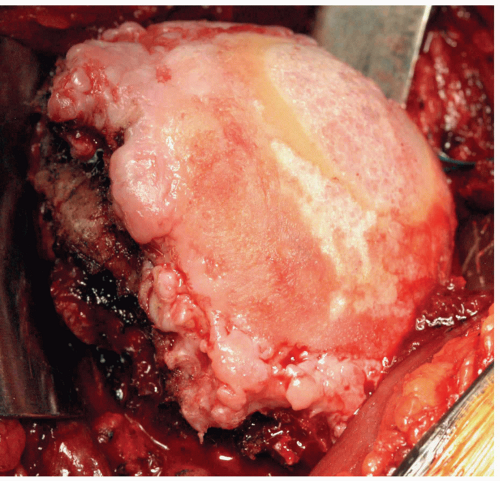 FIGURE 12-7. Osteoarthritis: Humeral head at the time of total shoulder arthroplasty. Flattening and enlargement of the humeral head is seen. Large proliferative osteophytes are noted circumferentially with inferomedial predominance, the “goat’s beard.” Punctate cystic lesions dot the eburneous bone. |
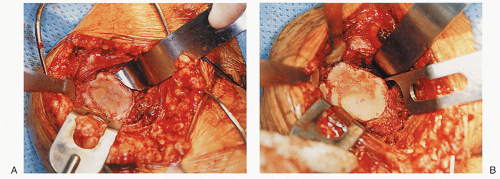 FIGURE 12-8. Osteoarthritis: Glenoid at the time of total shoulder arthroplasty demonstrating (A) demarcation between intact anterior cartilage and posterior eburneous subchondral bone. Peripheral osteophytes are seen. (B) Significant circumferential osteophyte formation. |
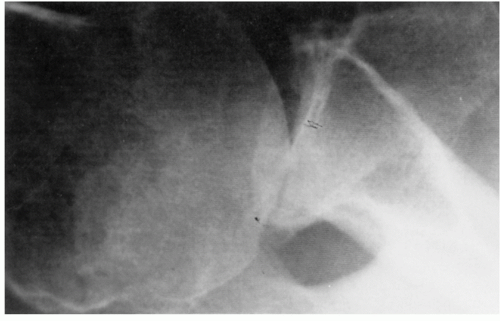 FIGURE 12-9. Osteoarthritis: Axillary lateral view demonstrating preservation of the anterior cartilage, posterior subluxation of the humeral head, and preferential wear of the posterior aspect of the glenoid. |
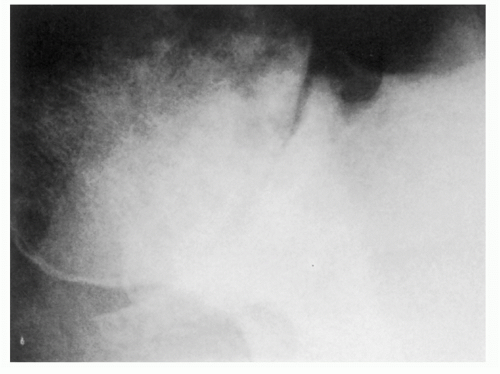 FIGURE 12-10. Osteoarthritis: Enlargement of the glenoid without evidence of significant preferential posterior wear. |
 FIGURE 12-11. Osteoarthritis: Osteocartilaginous bodies are seen in the subscapularis bursa and in an unusually exaggerated inferior recess of the glenohumeral joint. |
tissue contractures or pain, optimum films are sometimes not possible to obtain. In those instances, a CT scan will prove extremely useful in assessing glenoid morphology, glenohumeral relations, the presence of osteocartilaginous bodies, and the estimation of the anatomic version (Fig. 12-13).39 The accuracy of version determination, wear orientation, and estimation of extent of glenoid bone loss is enhanced by proper orientation of the scapula, three-dimensional reconstruction, and a sophisticated method of computer-generated modeling of the glenoid vault.87,256,342,723,724 and 725 Other findings of osteoarthritis are densification of subchondral bone, subchondral cysts, and peripheral osteophytes along the glenoid margins and adjacent to the articular surface of the humeral head, especially inferiorly. The humeral head may be flattened and enlarged. A triple-phase bone scan may prove beneficial for confirmation of disease localization when the plain films show no or early changes of glenohumeral arthritis (Fig. 12-14). The role of ultrasonography is uncertain although its utility for the detection of synovitis is recognized.322,400 The routine use of MRI for disease detectable by plain films would be considered exotic. However, it may have a role as a screening tool in pre-radiographic or early disease, to detect synovitis, to quantify articular cartilage volume, thickness and/or to monitor response to nonsurgical therapeutic interventions.44,97,322,496
 FIGURE 12-12. Osteoarthritis: Significant loss of external rotation is seen before total shoulder arthroplasty. |
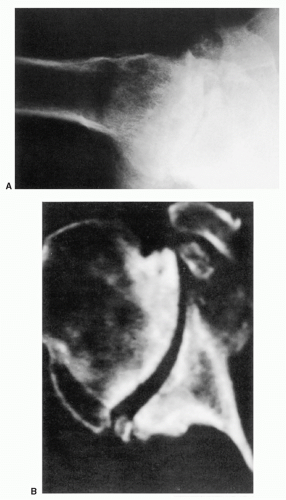 FIGURE 12-13. Osteoarthritis: (A) Findings on axillary lateral view may fail to define the pathoanatomy with accuracy. (B) Significant deformity noted on computed tomography scan. Loose bodies have attached to the anterior glenoid. External rotation limitation can be appreciated, due to contact of the posterior humeral head and osteophyte against the glenoid. |
Petty provided the initial publication that cited chondrolysis in association with shoulder arthroscopy and thermal energy.628 Reports of severe chondrolysis appeared more frequently thereafter.95,134,147,282,373,465,483 The effect of thermal energy on articular cartilage has been investigated.391,479,480,481 and 482
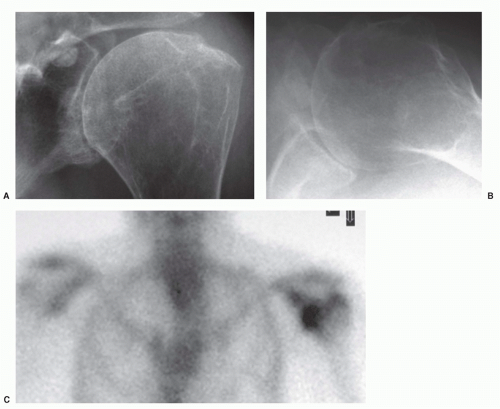 FIGURE 12-14. (A,B) Plain radiographs of mild glenohumeral osteoarthritis. (C) Delayed phase of bone scan with increased uptake of radionuclide in the glenohumeral joint. |
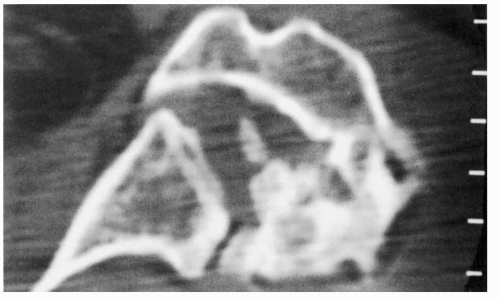 FIGURE 12-15. Posttraumatic osteoarthritis: Changes resulting from proximal humerus fracture, demonstrating joint incongruity and loss of humeral articular surface. |
recurrent glenohumeral instability. A late debilitating sequela to glenohumeral instability and its surgical treatment was, in one form, first appreciated by Hindmarsh and, in another form, initially observed by Neer.335,571 The term “dislocation arthropathy” spawned and included those occurrences of glenohumeral arthritis with a well-documented history of glenohumeral dislocation, often in patients having undergone surgical treatment (Fig. 12-20).572,715 Whether it is an essential consequence of glenohumeral instability, as suggested by Hovelius, is unknown.352
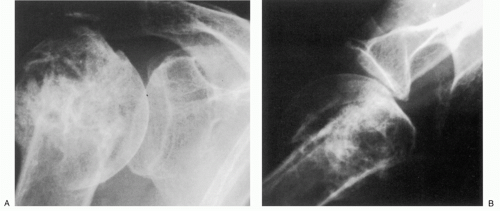 FIGURE 12-16. (A,B) Posttraumatic arthritis. Proximal humeral malunion with distortion of proximal humeral anatomy. Early arthritic changes are observed. Dysvascular changes are not present in the articular segment. |
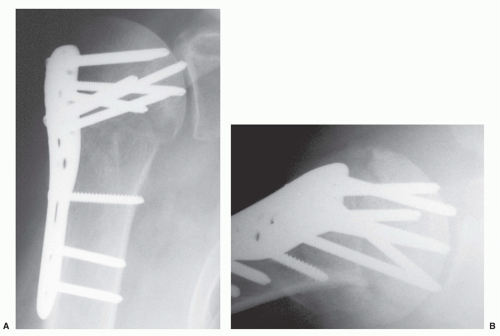 FIGURE 12-17. (A,B) Proximal humeral internal fixation screws violate the subchondral bone of the humeral head. (C) The thickness of the humeral head cartilage is insufficient to prevent the tips of the screws from projecting “proud” into the glenohumeral joint. (D) In this instance, the cause of posttraumatic osteoarthritis is obvious: the destruction of glenoid and humeral head articular cartilage by screws that were too long. |
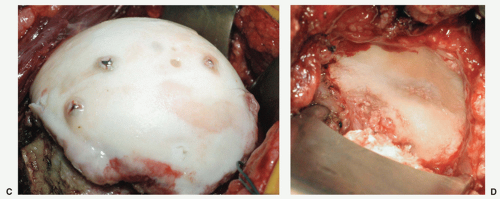 FIGURE 12-17. (Continued) |
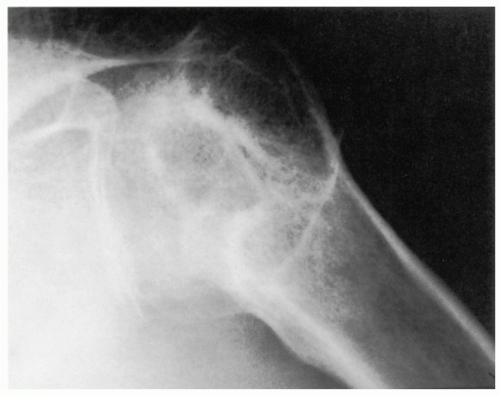 FIGURE 12-18. Posttraumatic arthritis: Malunited proximal humerus fracture leading to advanced disease. |
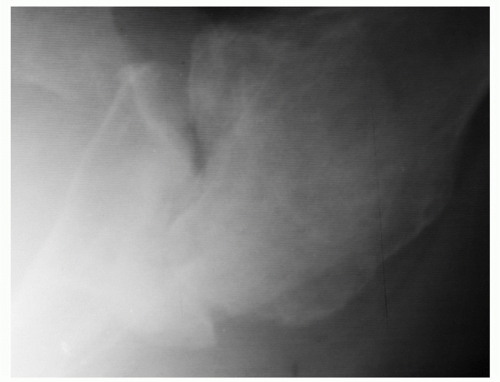 FIGURE 12-19. Posttraumatic arthritis: Chronic locked posterior dislocation with gross incongruity of the glenohumeral joint. |
and surgical treatment correlated with the preoperative development of arthritis.11,99,349,715,759 Marx noted that the glenohumeral dislocation requiring reduction was found to be associated with a 10- to 20-fold increase in the risk for the subsequent development of severe arthrosis sufficiently severe to warrant shoulder arthroplasty.505
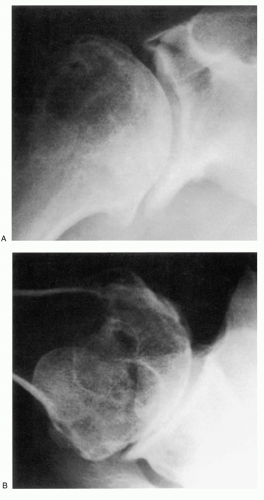 FIGURE 12-20. (A,B) Arthritis of dislocation: The sequelae to two previous surgeries, including anterior stabilization and subsequent staple removal. |
nearly 20% of patients.99 Once again, age at the time of the initial instability episode seemed to be most important for the subsequent development of arthritis. Other important factors were age at the time of surgery and a longer interval of follow-up. In contrast to Rachbauer, the presence of arthritis was influenced by the number of instability episodes prior to surgery.655 The findings regarding decreased external rotation were inconclusive. Considering these observations, Buscayret suggested that surgery does not influence the risk factors nor prevent the development of arthritis in shoulders that undergo attempts at surgical stabilization.99 Ogawa et al. stated more emphatically, “…unquestionably apparent that no operative procedure prevents development of OA.”599 Additionally, the arthritis they recognized postoperatively had developed before surgical stabilization.
dislocation suggests a direct relation between the forces dissipated to the articular cartilage and the restraining soft tissues. In the so-called “tight” shoulders, higher forces may be necessary for traumatic dislocation, whereas more lax shoulders require less force. The development of postdislocation arthrosis may result from recurrent episodes of instability because eccentric loading during pathologic translocation transmits greater shear and compression forces at the articular interface. Progressive bone loss in the anteroinferior quadrant, in addition to the loss of the labrum, was found to have the effect of causing further increase in mean contact pressures and peak pressures and a decrease in contact area across the glenohumeral joint.291 It is possible that surface imperfections and impression fractures of the humeral head could further damage the articular cartilage with each successive dislocation event. The resultant accumulations of particulate joint debris and newly formed osteocartilaginous loose bodies could theoretically contribute a third body wear mechanism. These detrimental effects could coexist and become additive in their potential for joint destruction.
 FIGURE 12-21. Arthritis of dislocation: The result of recurrent posterior glenohumeral instability. Note significant posterior humeral subluxation and eccentric wear of the posterior two-thirds of the glenoid. |
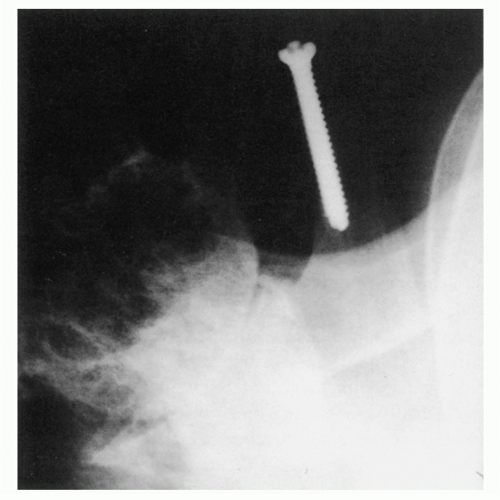 FIGURE 12-22. Arthritis of dislocation: Capsulorrhaphy arthropathy with significant deterioration of the glenohumeral articulation, total loss of joint space, and secondary changes within the humeral head. |
of motion.612 Some have had multiple surgical procedures. Despite mild to moderate radiographic changes of arthrosis, the clinical impact, in some instances, is negligible.113
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


