Pain Signaling Systems from Injured Cervical Facet Joints
Meagan E. Ita
Beth A. Winkelstein
Chronic pain is a common symptom of whiplash-associated injuries. During whiplash, the spine undergoes abnormal motions, and tissue injury of the capsular ligament of the cervical facet joints occurs. Under such pathophysiological loading, peripheral and central neuroimmune and nociceptive signaling cascades are initiated that lead to the onset and maintenance of pain (Fig. 2-1). Pain sensation includes both sensory and emotional experiences, but “nociception” refers to the physiological responses and signal transmission that encodes pain [33]. Typical behavioral signs and symptoms are exhibited by whiplash patients, with allodynia and hyperalgesia to mechanical and thermal stimuli. Allodynia is that pain elicited by a normally non-noxious (nonpainful) stimulus, and hyperalgesia is a heightened response to a noxious (painful) stimulus [33]. These signs are quantifiable and have been used in both clinical studies and animal models of pain, using dermatomal mapping between species. When considering whiplash, the term “injury” is complicated since it may apply to structural injury of tissue in terms of biomechanics, or it may be taken as dysfunction or pain when considering physiological metrics. For the purposes of clarification in this chapter, injury encompasses scenarios in which there is pain. Further, the development of facet-mediated
whiplash pain symptoms following injury depends on a host of neuroimmune cascades and nociceptive signaling responses, as well as on the magnitude of biomechanical loading of the facet capsule (Fig. 2-1).
whiplash pain symptoms following injury depends on a host of neuroimmune cascades and nociceptive signaling responses, as well as on the magnitude of biomechanical loading of the facet capsule (Fig. 2-1).
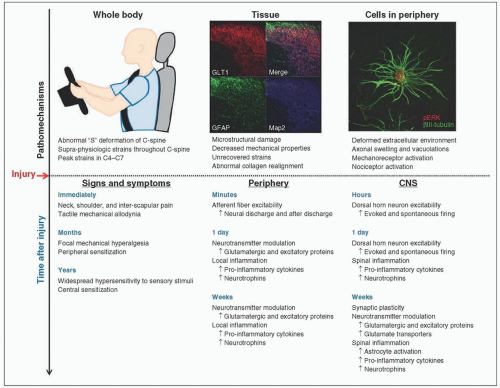 FIGURE 2-1 The pathomechanisms and resulting spatiotemporal local and central physiological responses due to facet joint injury from whiplash have been defined using a host of models, ranging from cadaveric and human models to in vitro cellular-based systems. Taking those collections of work together, an overall schema can be constructed spanning a range of size- and time-scales. Clinical reports, together with biomechanical studies, support a characteristic neck injury profile that induces local injuries throughout the cervical spine (C-spine), and the facet joint in particular. Those local injuries to the collagen and afferents of the facet capsular ligament produce neuroimmune cascades in the periphery and CNS that depend on the facet tissue mechanics and contribute to the onset and maintenance of pain. |
This chapter provides an overview of the relationships between biomechanical loading, nociceptive signaling, and pain to describe the relevant physiological responses of the facet joint to mechanical loading in the context of pain, ranging from macroscopic points of view to cellular injuries (Fig. 2-1). It begins with a review of clinical studies summarizing the epidemiology related to cervical facet joint pain from whiplash, and describing those related pain symptoms and the time course of the clinical pain syndrome. Next, biomechanical studies are briefly reviewed, including those of volunteers, full-body cadavers, and cadaveric head-neck preparations; of note, that body of work is quite extensive and far greater than what can be reviewed here [20].
The engineering evidence that implicates the facet joint as having a role in whiplash injury and pain is summarized here. Building off that work, in vivo models are reviewed, particularly those that incorporate biomechanics to understand mechanisms of pain production. In that section, we relate findings regarding pain symptoms with the physiological cascades in both the periphery and the central nervous system (CNS); more exhaustive reviews are provided [6]. Nociceptive signaling can lead to sensitization, which is increased responsiveness of neurons to their normal input or recruitment of a response to normally subthreshold inputs [33]. Sensitization can occur in the periphery or in the CNS. Peripheral sensitization leads to altered nociceptive responses at the injury site, including decreased thresholds for afferent firing and increased responsiveness of peripheral nociceptive neurons; central sensitization involves the increased spontaneous activity and responsiveness of nociceptive neurons in the CNS, which results in increased nociception at secondary sites that have no tissue damage [33]. Given the challenges in measuring ligament damage other than gross tissue responses in vivo, we separately present studies that further investigate local mechanotransduction processes by highlighting relationships between locally induced biomechanical deformations and microstructural changes, and the release of pain mediators. Lastly, we conclude this chapter with a brief section highlighting the importance of some of these findings for pain therapies and interventions
that specifically target those spatiotemporal neuroimmune cascades that are related to facet-mediated pain. We briefly propose several future directions for research that will further define facet-mediated pain signaling and whiplash mechanisms that can further inform effective clinical diagnostics and treatments.
that specifically target those spatiotemporal neuroimmune cascades that are related to facet-mediated pain. We briefly propose several future directions for research that will further define facet-mediated pain signaling and whiplash mechanisms that can further inform effective clinical diagnostics and treatments.
Neck pain is a common and costly medical problem worldwide, and affects around 100 million American adults, with an estimated annual economic cost in the United States of up to $635 billion [18]. Neck pain is the most common symptom reported by patients sustaining whiplash injury, with one-third of whiplash patients reporting symptoms that last for at least 2 years following injury [37]. The cervical facet joints are bilateral joints in the posterolateral region of the spine, and are responsible for coupling rotation and bending in the neck, as well as transmitting axial load [20]. The articulating joint is innervated by the medial branches of the primary dorsal rami of the superior and inferior cervical levels of each joint [3]. Afferent nerve fibers terminate in the facet joint capsule; these include mechanoreceptive and nociceptive C- and Aδ- fibers, with cell bodies in the dorsal root ganglion (DRG) that transmit sensory information from the periphery and terminate in the dorsal horn of the spinal cord [4, 6, 20, 21]. As such, because the facet capsular ligament is rather weak and the facet joint can undergo abnormal motions during whiplash, the facet joints and their capsular ligaments have the potential to generate pain under certain loading conditions.
Patients sustaining whiplash injuries present with pain symptoms and widespread hypersensitivity to mechanical and thermal stimuli that are indicative of CNS sensitization [36, 47, 49]. Pain symptoms from whiplash injury include neck pain and stiffness and have early onset after injury, with many that can persist for at least 2 years [36]. Whiplash patients also exhibit decreased pain thresholds to pressure stimuli over the articular pillars of the cervical spine and in the upper limbs, decreased thermal pain thresholds over the cervical spine, and
hypersensitivity during upper limb extension [47, 49]. For example, in a study of 76 whiplash patients, 22.4% of patients reported persistent moderate/severe pain symptoms and demonstrated generalized hypersensitivity to sensory stimuli, which was distinguishable from patients who reported recovered or mild pain [49]. Additionally, while all of those whiplash patients exhibited behavioral sensitivity at 1 month after injury, hyperalgesia persisted at the same severity level for at least 2 years in patients with persistent moderate/severe pain, but it resolved in all of the other patients within 2 months after injury [49]. The existence of localized and focal mechanical hyperalgesia in all whiplash patients early after injury suggests peripheral sensitization of nociceptors, while the generalized hypersensitivity that long outlasts the injury event is likely due to central sensitization.
hypersensitivity during upper limb extension [47, 49]. For example, in a study of 76 whiplash patients, 22.4% of patients reported persistent moderate/severe pain symptoms and demonstrated generalized hypersensitivity to sensory stimuli, which was distinguishable from patients who reported recovered or mild pain [49]. Additionally, while all of those whiplash patients exhibited behavioral sensitivity at 1 month after injury, hyperalgesia persisted at the same severity level for at least 2 years in patients with persistent moderate/severe pain, but it resolved in all of the other patients within 2 months after injury [49]. The existence of localized and focal mechanical hyperalgesia in all whiplash patients early after injury suggests peripheral sensitization of nociceptors, while the generalized hypersensitivity that long outlasts the injury event is likely due to central sensitization.
The facet joints have been implicated as the leading source of pain in patients with chronic whiplash-associated pain in 25-62% of cases via anesthetic nerve blocks or provocative testing [1, 2, 15, 16]. For example, 82 of 128 patients with chronic neck pain who underwent diagnostic blocks to the cervical facets were completely relieved of pain [1]. Pain symptoms are also attenuated by radiofrequency neurotomy, which denervates the cervical facet joints through simulation of the medial branches that innervate them [2]. Provocative testing via joint distension or electrical stimulation of cervical facet joints can also reproduce patient pain in the occiput, neck, and/or shoulders [15, 16], which confirms that mechanical loading of the capsule can activate its nociceptive afferents. These studies reveal the cervical levels most commonly implicated in facet-mediated chronic pain as C2-C3, C5-C6, and C6-C7 [2].
Studies with human volunteers, full-body and/or head-neck cadaveric specimen preparations simulating low-velocity rear-end motor vehicle impacts that are characteristic of the whiplash exposure have
collectively defined a signature deformation of the cervical spine. That deformation is initiated within the first 100-120 ms after seat acceleration due to the upward motion of the thorax, which transmits loads to the cervical spine, producing an “S” curvature of the spine [17, 23, 35, 39, 57]. During that whiplash neck kinematic, the lower cervical levels undergo hyperextension and tension anteriorly, while the upper cervical levels undergo flexion [17, 57]. The local intervertebral motions that result from abnormal cervical deformations can induce excessive strains in the cervical facet capsules and other spinal ligaments, with magnitudes that vary across the spinal levels [20]. The strains in the cervical facet capsules are greatest in the lower cervical spine (C4-C7) [9, 17, 40, 41, 50], with the linear strains across the C6/C7 facet joint peaking at 29-40% during accelerations that simulate moderate-to-severe whiplash-associated motor vehicle impacts [41]. Further, for a comparable injury exposure, the lower cervical facets slide anteriorposteriorly parallel to the line of the joint articulation, reaching a maximum relative displacement of 6.0 mm (˜51% facet capsular strain as inferred from bony landmarks) [9]. In cadaveric simulations of head restraint contact during rear impacts, the C4/C5 and C5/C6 facets undergo the greatest combined anterior-posterior, superior-inferior displacements of 2.5 ± 1.8 and 2.5 ± 2.3 mm, respectively [50]. Similar translations measured between upper and lower bony facet landmarks have been reported for studies of cadaveric head-neck preparations, with C4/C5 and C6/C7 experiencing the greatest anterior-posterior (5.4 mm) and superior-inferior (2.6 mm) displacements, respectively [41].
collectively defined a signature deformation of the cervical spine. That deformation is initiated within the first 100-120 ms after seat acceleration due to the upward motion of the thorax, which transmits loads to the cervical spine, producing an “S” curvature of the spine [17, 23, 35, 39, 57]. During that whiplash neck kinematic, the lower cervical levels undergo hyperextension and tension anteriorly, while the upper cervical levels undergo flexion [17, 57]. The local intervertebral motions that result from abnormal cervical deformations can induce excessive strains in the cervical facet capsules and other spinal ligaments, with magnitudes that vary across the spinal levels [20]. The strains in the cervical facet capsules are greatest in the lower cervical spine (C4-C7) [9, 17, 40, 41, 50], with the linear strains across the C6/C7 facet joint peaking at 29-40% during accelerations that simulate moderate-to-severe whiplash-associated motor vehicle impacts [41]. Further, for a comparable injury exposure, the lower cervical facets slide anteriorposteriorly parallel to the line of the joint articulation, reaching a maximum relative displacement of 6.0 mm (˜51% facet capsular strain as inferred from bony landmarks) [9]. In cadaveric simulations of head restraint contact during rear impacts, the C4/C5 and C5/C6 facets undergo the greatest combined anterior-posterior, superior-inferior displacements of 2.5 ± 1.8 and 2.5 ± 2.3 mm, respectively [50]. Similar translations measured between upper and lower bony facet landmarks have been reported for studies of cadaveric head-neck preparations, with C4/C5 and C6/C7 experiencing the greatest anterior-posterior (5.4 mm) and superior-inferior (2.6 mm) displacements, respectively [41].
Despite being of greater magnitude than those experienced during physiological neck motions, whiplash-induced strains in the cervical facet capsules are not sufficient to induce capsule rupture [40, 41, 56]. In addition, the intervertebral rotations at C6/C7 and C7/T1 during simulated whiplash exceed the physiological limits of rotation [17], with ligament laxity occurring throughout the cervical spine [19] but no evidence of capsule rupture [17, 40, 41, 48, 56]. Interestingly, facet capsule rupture itself, despite being more severe biomechanically, does not induce pain [55]. Taken together with the fact that the facet capsule is richly innervated with mechanosensitive afferents [3, 4, 21], the absence of pain after joint rupture implies that such
joint afferents must be intact at injury for facet-mediated pain to develop from facet joint trauma.
joint afferents must be intact at injury for facet-mediated pain to develop from facet joint trauma.
During whiplash, capsular deformations are not uniform throughout the cervical spine or regionally on the surface of the capsular ligament. For example, deformations are greatest in the posterior portion of the capsule relative to the anterior portion [50]. Capsular strains are also nonuniform during cervical spine bending, although the principal strains are typically directed along the joint line [54]. Nonuniform strains in the facet capsule have important implications for the mechanosensitive afferents that terminate in that capsule since higher magnitude strains may preferentially activate or injure fibers in specific regions. If these higher magnitude strains load the facet capsule while it remains intact, and thus do not rupture the afferents themselves, a biomechanical environment is created by that subfailure loading condition that has the capacity to generate pain.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


