Overuse Syndrome
Jess H. Lonner
Eric B. Smith
 A 43-year-old slightly overweight man who has not participated in vigorous physical activity in many years has begun bicycling for the past few weeks. He doesn’t stretch or warm up prior to exercising and presents 2 days after his last ride with severe generalized right knee pain and difficulty walking. He denies any discrete history of traumatic injury. |
CLINICAL PRESENTATION
The general terms overuse syndrome or overuse injury refer to musculoskeletal pain or dysfunction that is the result of any physical activity that exceeds the strength of musculoskeletal tissues such as bone, tendons, ligaments, joints, or bursae.1 Such activity causes microtrauma to these structures and results in pain and dysfunction that can be severe. The knee joint is not immune to this. The diagnosis of overuse syndrome must be entertained in any active individual with knee pain after heavy physical activity with no discrete history of trauma. Overuse can cause tendinitis (quadriceps, patellar, hamstrings, gastrocnemius, iliotibial band syndrome, etc.), capsulitis, periostitis, bursitis, or stress fractures.
Pain is often achy and most pronounced 1 to 2 days after intense physical activity, particularly when the patient has not warmed up or stretched.
CLINICAL POINTS
Tissue pain and dysfunction may be severe.
Pain is frequently achy.
Vigorous physical activity with no distinct history of trauma may trigger the syndrome.
PHYSICAL FINDINGS
Physical findings in patients with knee overuse injuries are many and varied. Pain may be vague and poorly localized. However, the underlying structures that have suffered microtrauma will often be tender and inflamed, including the hamstrings, quadriceps, patellar tendon, iliotibial band, and the pes anserinus. Stretching these structures passively or providing resistance to active contraction during physical exam will elicit pain in the affected tissue.
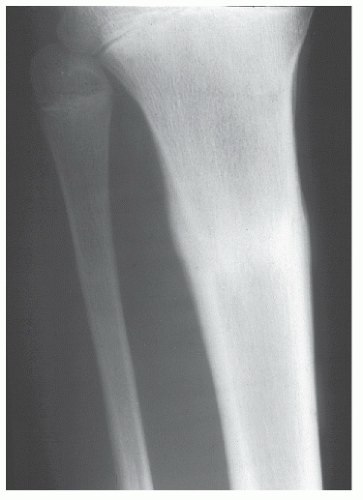
Overuse stress fractures may be present in any bony structures about the knee, most commonly the anterior medial tibia. Patients with stress fractures will have focal point tenderness over the affected bone.
STUDIES (LABS, X-RAYS)
Radiographs are often nondiagnostic, even early in a stress fracture. Magnetic resonance imaging or bone scan should be obtained if there is suspicion of stress fractures or avascular necrosis (Fig. 17-1).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


