Occipitocervical Fixation and Fusion
Andrew H. Milby
John M. Rhee
Illustrative Case
A 51-year-old male presented to us with numerous craniocervical developmental abnormalities and severe cervical myelopathy because of occipitocervical assimilation, basilar invagination, and C1-2 instability. He was admitted for preoperative cervical traction, which provided partial reduction of the basilar invagination (Figures 8-1 and 8-2).
 Figure 8-1 ▪ Preoperative neutral lateral x-ray of cervical spine. Note the severe basilar invagination of the odontoid, which is not only proximally but also dorsally displaced into the foramen magnum. Mutliple auto-fusions are noted, as well as a congenital assimilation of C1 to the occiput (note absence of visible C1 posterior arch). |
 Figure 8-2 ▪ Lateral x-ray of craniocervical junction in Gardner-Wells tongs traction demonstrating partial reduction of basilar invagination. |
Indications
Unstable traumatic fractures or ligamentous injuries of the craniocervical junction.
Myelopathy due to basilar invagination from inflammatory, infectious, or neoplastic causes.
Adjunct fixation in long cervical constructs with concern for proximal fixation failure because of limited available fixation points and/or poor bone quality.
Radiologic Assessment
Carefully assess vertebral arteries for any anatomic variation and to determine safe zones for exposure and instrumentation at upper cervical levels (Figure 8-3).
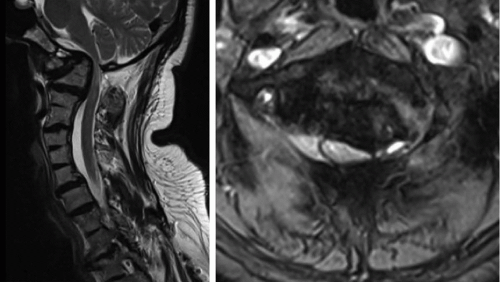
Figure 8-3 ▪ Sagittal T2-weighted MR image, demonstrating severe cord compression with atrophy and myelomalacia at the occipitocervical junction.
Review intracranial imaging (axial CT cuts through the occiput) for locations of dural sinuses and variations in occipital anatomy (Figures 8-4 and 8-5).
Measure approximate lengths and sizes of planned occipital and cervical instrumentation.
Determine extent of suboccipital decompression, if indicated.
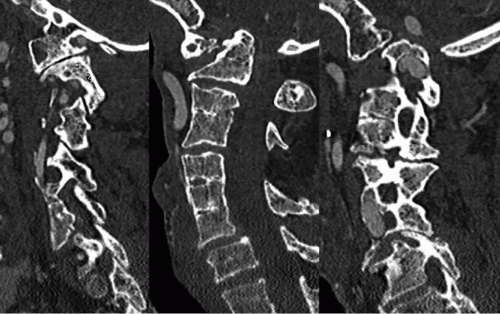 Figure 8-4 ▪ Sagittal CT angiogram images demonstrating C1-2 subluxation, invagination of the dens, multiple Klippel-Feil segments, and facet auto-fusions. Note the vertebral artery anomaly (right) significantly narrowing the C2 pars and precluding screw placement. |
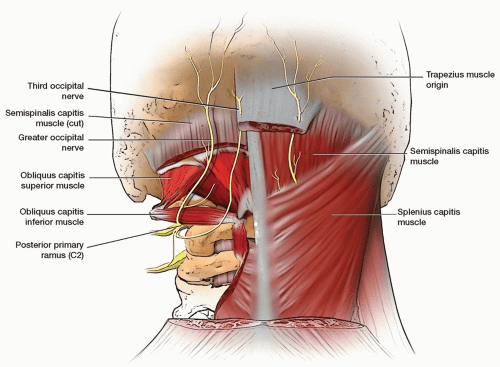 Figure 8-5 ▪ Anatomic diagram illustrating course of greater occipital nerve. |
Special Equipment
Occipitocervical instrumentation
C-arm
Positioning
Related posts:
 Cervical Subaxial Laminectomy, Instrumentation, and Fusion (C3 to Upper Thoracic)
Cervical Subaxial Laminectomy, Instrumentation, and Fusion (C3 to Upper Thoracic)
 Costotransversectomy and Lateral Extracavitary Approach
Costotransversectomy and Lateral Extracavitary Approach
 Lumbar Corpectomy
Lumbar Corpectomy
 Minimally Invasive Transforaminal Lumbar Interbody Fusion
Minimally Invasive Transforaminal Lumbar Interbody Fusion
 Airway Complications After Anterior Cervical Diskectomy and Fusion/Cricothyrotomy
Airway Complications After Anterior Cervical Diskectomy and Fusion/Cricothyrotomy
 Operative Treatment of Hangman’s Fractures
Operative Treatment of Hangman’s Fractures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


