Minimally Invasive Reduction and Fixation Techniques for Acetabular Fractures
Gil R. Ortega
Hrayr G. Basmajian
INDICATIONS
Letournel and Judet1 have demonstrated approaches to adequately open reduce and stabilize acetabular fractures. Their work as well as other authors’ work has emphasized the importance of anatomical reduction and how an acetabular fracture anatomical reduction can lead to long-term satisfactory results.2, 3, 4, 5 and 6 Some open approaches are associated with significant risks including infection, wound healing, neurovascular injury, heterotopic ossification, femoral head avascular necrosis, and thromboembolic events.2, 3, 4 and 5,7,8 Many of these risks are associated with the approach rather than the fixation or injury.
With the advent of improved imaging techniques including fluoroscopy and computed tomography (CT) imaging, there have been advancements in acetabular surgery reduction and internal fixation techniques. Appropriate internal fixation of acetabular fractures permits early ambulation and can significantly reduce the amount of time spent in bed.1 Some authors agree that anatomic reduction and internal fixation are the goals of all acetabular surgery.2,3,5,7,8 The goals when using minimally invasive techniques should include obtaining the best reduction and stable internal fixation. The following situations are described indications in the literature and also what surgeons may use when deciding between a formal open procedure and potential indications.6,9, 10, 11 and 12
Fracture Patterns
Any fracture in which an anatomic reduction can be obtained and stabilized with available methods
Nondisplaced (1 to 3 mm) and potentially unstable fractures
Minimally displaced (3 to 5 mm) with a fracture gap but no step-off
Transtectal fractures with medial roof-arc angle (AP radiograph) of 45 degrees or less13
Minimal comminution and no free fragments in the hip joint (Parker)20
Unstable fractures as demonstrated with validated stress examinations15
Both column fractures with acceptable secondary congruence
Patient Factors
Patients deemed too sick to withstand an extensive open procedure with risk of substantial blood loss
Obese patients at high risk of complications with open procedures16
Patients with Morel-Lavallee lesions or compromised skin around planned open procedure
Geriatric patients with pre-existing symptoms of arthritis
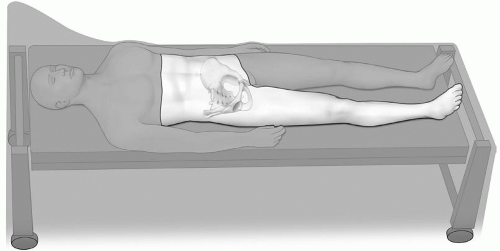 Figure 9.1 Photo demonstrating operative zone for minimally invasive acetabular surgery. |
PATIENT POSITIONING
When attempting or considering minimally invasive surgery of the acetabulum, the surgeon must always be familiar and prepared to convert to an open procedure, if required. Generally, patients are positioned supine on a radiolucent operating room table. The surgeon may prepare the operating room table with traction apparatus setup in order to use skeletal traction if required. The operative zone should include the pelvis and at least the ipsilateral lower extremity (Fig. 9.1). The operative zone allows the surgeon to perform many reduction maneuvers as well as internal fixation of anterior column, posterior column, and both column fractures. We find it very important to communicate with our department of radiology and ensure that the radiology technician is familiar with the surgery and the necessary fluoroscopic views.6 Before surgical prepping of the operative zone, the surgeon should routinely obtain practical fluoroscopic views to ensure the entire bony anatomy may be seen by fluoroscopy. The surgeon must also ensure that there is no contrast material present within the bladder that might obscure images.12
STRESS EXAMINATION OF ACETABULAR FRACTURES
Deciding on when not to operate on an acetabular fracture can be a difficult and sometimes an unclear decision. Most authors agree that this decision depends upon a congruent joint under the acetabular roof and a stable intact roof.5,7,13,15,17 Matta et al.7 first described the idea of roof arc measurements and later used CT to quantify the amount of acetabular roof recommended to be intact to treat nonoperatively.13 Posterior wall fractures do not apply to these measurements and stability is the most crucial factor for these injuries. Studies have shown that when less than 20% of the posterior wall was fractured, hips were stable, and when the fracture involved greater than 50% of the posterior wall, they were unstable.18,19 This leaves a fairly large gray area with room for measurement error. Tornetta15 described the use of dynamic stress examinations to evaluate all patients they considered for nonoperative treatment. In this study, which also included patients with documented dislocations, they
examined all patients under anesthesia. They described internally and externally rotating the affected hip in flexion, extension, and abduction; at each position an AP, iliac oblique, and obturator oblique image was examined for incongruence. Also, a stress “sufficient to rock the patient on the table … in the direction of displacement” was then applied. In their report, 3 of their 41 patients demonstrated a loss of congruence and were treated operatively. At a follow-up of 2.7 years, 91% of their patients had good or excellent results.
examined all patients under anesthesia. They described internally and externally rotating the affected hip in flexion, extension, and abduction; at each position an AP, iliac oblique, and obturator oblique image was examined for incongruence. Also, a stress “sufficient to rock the patient on the table … in the direction of displacement” was then applied. In their report, 3 of their 41 patients demonstrated a loss of congruence and were treated operatively. At a follow-up of 2.7 years, 91% of their patients had good or excellent results.
SURGICAL APPROACHES, FIXATION AND REDUCTION TECHNIQUES
For minimally invasive techniques to be successful the goals of each surgery must be considered as each fracture and patient physiology may be different. In acetabular surgery, the reduction remains the most critical aspect of any minimally invasive surgery. The inability to reduce the fracture continues to be the major critique of its opponents. It can be challenging if not impossible for surgeons to obtain an anatomic reduction using minimally invasive methods. Therefore, the surgeon must consider which fractures and patients may benefit from a minimally invasive technique or a formal open reduction and internal fixation procedure. One instance where minimally invasive techniques may be an option is in elderly patients as it has been demonstrated that elderly patients can tolerate imperfect reductions better than younger patients.20
For most minimally invasive acetabular procedures, surgery is best accomplished within a few days from injury.6,10, 11 and 12,14 Many times the reduction can be as straightforward as traction or rotation of the leg. Several reduction tools such as Schanz pins, ballpoint pushers, and reduction clamps are necessary for fracture reduction maneuvers (Fig. 9.2). Mini-lateral windows can assist in accessing an anterior column or posterior column fracture, and using appropriate clamps the fracture can be reduced and stabilized. At times, it may be helpful to use a universal distractor (Synthes, Paoli, PA) to help reduce and hold a fracture prior to internal fixation.
 Figure 9.2 A: Reduction tools and instruments used in minimally invasive acetabular surgery (first four from left are cannulated “Pig Stickers” with offset and straight variety, middle black four are long elevators and/or reduction tools, last four on right are solid “Pig Stickers” with offset and straight variety with varying sharpness to tips, top image is large pelvic reduction clamp). B: Collinear clamp can be used in minimally invasive techniques (Synthes, Paoli, PA). C: Pelvic model and collinear clamp demonstrating example for reduction of quadrilateral plate and path to hold with wire placed through collinear clamp. |
ANTERIOR COLUMN FRACTURE REDUCTION AND INTERNAL FIXATION
The anterior column screw can be inserted in a retrograde or antegrade fashion. An anterior column screw may be used in a majority of anterior column fractures. Routt et al.21 first described the technique in which they used this screw in a retrograde manner after an open incision to treat pelvic ring injuries. Starr et al.12 also demonstrated using an anterior column screw in either antegrade or retrograde fashion for anterior column fixation.
For placement of an anterior column screw, the patient is placed supine (can also be done in lateral position, but antegrade only) with a small bump under the sacrum if necessary. A small bump may be necessary to elevate the pelvis to assist hand positioning when drilling and placing an anterior column screw. For improved access, we use the fluoroscopic C-arm on the ipsilateral side as the fracture for retrograde placement and the contralateral side for antegrade placement. During the insertion of the anterior column screw, two main views are used and checked: An inletiliac view and an outlet-obturator view (Fig. 9.3) as described.12,21 The former is to ensure that the wire does not perforate the inner cortex and injure the bladder or deviate anteriorly toward the vessels. The latter ensures that the wire avoids the hip joint and does not escape superiorly. These views are obtained by rotating either 20 degrees from standard inlet/outlet x-rays in a lateral oblique manner for an outlet-obturator x-ray and in a medial manner for an inlet-iliac x-ray.
The starting point for an anterior column screw is in-line from the greater trochanter to the thick part of the iliac crest, usually 4 to 5 cm posterior to the anterior-superior iliac crest in thin patients. A starting point just cephalad is used in smaller patients, whereas in obese or muscular patients, a point closer to the iliac crest is used.12 When the surgeon uses a cannulated guide with a sharp point, he may place the drill or wire securely into bone without slipping from the highly sloped bony surface (Fig. 9.4). This cannulated guide may be used for most of the techniques described in this chapter.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


