stimuli. An example of chronic nociceptive pain is rotator cuff injury.23 This pain may be intermittent, localized, and related to position and weight-bearing or physical activity. In severe, long-standing cases, it may be persistent, diffuse, and nonrelated to position of the extremity of its mobility. Nociceptive pain is common among chronic shoulder pain.
 FIGURE 37-1. Relationship between sympathetically maintained pain and some selected painful conditions. This illustration is intended as a conceptual framework without indication of the quantitative relationship between the intersections. Various pain disorders may have a component of sympathetically maintained pain. |
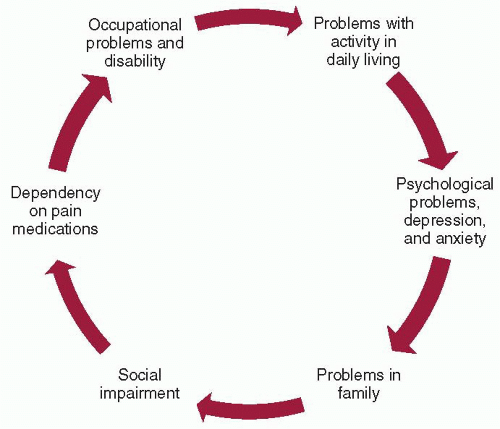 FIGURE 37-2. Relationship between various components of chronic pain disorder. |
TABLE 37-1 Pharmacologic Classifications of Nonsteroidal Anti-inflammatory Drugs | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
A twofold increase in acute myocardial infarction with rofecoxib compared to placebo prompted the voluntary withdrawal of rofecoxib (Vioxx) from the U.S. and worldwide markets in 2004. The same year, the U.S. Food and Drug Administration (FDA) requested Pfizer, Inc., to voluntarily withdraw Bextra (valdecoxib) from the market. This request was based on the lack of adequate data on the cardiovascular safety of long-term use of Bextra, increased risk of adverse cardiovascular events in short-term coronary artery bypass surgery trials, and reports of serious and potentially life-threatening skin reactions. The FDA has also asked manufacturers of all prescription NSAIDs, including Celebrex (celecoxib), a COX-2 selective NSAID, to revise the labeling to include a boxed warning to highlight the potential cardiovascular and GI risks.
PHM and painful diabetic neuropathy. Gabapentin has been used in different pain syndromes, including trigeminal neuralgia and painful tonic spasms associated with multiple sclerosis, reflex sympathetic dystrophy, painful HIV-related peripheral neuropathy, and neuropathic cancer pain, postpoliomyelitis pain, central dysesthetic pain following spinal cord injury and erythromelalgia, and headache syndromes.42,52
TABLE 37-2 Antiepileptic Medications for the Treatment of Neuropathic Pain | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


