Bone loss with ageing is universal and many will become osteoporotic in later life with increased risk of fracture. Measures therefore need to be taken by all to maximize bone mass and strength at all ages and to reduce risk of injuries when older. This needs to be at all stages of life. In this chapter we review the lifestyle interventions that all should follow to reduce risk at the population level. Some people are at greater risk and have most to lose if they do sustain a fracture and most to gain by preventative measures. For them, a more effective intervention may be appropriate. We have considered how to identify such individuals at most risk and in the next chapter chapter we review the evidence of what specific interventions will increase bone density and reduce fracture risk.
When assessing the evidence for the effectiveness of any intervention, there are several issues that need to be considered: (1) the characteristics of the study population compared with the target population; (2) the level of risk of the study population for sustaining a fracture; and (3) were the outcome measures used meaningful and standard? Bone density changes are a surrogate for the clinically relevant goal of fracture prevention. Studies to demonstrate fracture prevention have to be very large and over long periods of time and, as a consequence, data are deficient for some interventions. There are few comparative studies of the different treatments. For lifestyle risk factors, evidence of increased risk of osteoporosis or fracture does not mean that correcting the risk factor will necessarily reduce that risk – direct evidence of efficacy is needed although often the appropriate studies have not been done. A difficulty of epidemiological studies is that the various lifestyle factors are confounders of each other as, for example, many smokers also consume alcohol, are thin, and are less physically active. Concordance is very important when considering if an intervention will be effective in clinical practice in contrast to a clinical trial. This is very important when treatment has to be long term and there is no easily recognized clinical response to encourage the person to continue with treatment.
It is important to remember that treatment of osteoporosis is not just about prevention of another fracture. Many patients will have already sustained a fracture and they require optimal fracture management and rehabilitation to minimize the impact in the short and long term.
LIFESTYLE INTERVENTIONS
Increase in life expectancy is the result of increased economic wealth and improved health care from birth onwards. However, increased wealth has also brought lifestyle changes such as urbanization, a more sedentary way of living, poor diet, smoking, and alcohol abuse, which counteract bone health. Undernutrition in developing countries and the fashion for excessive thinness in westernized countries also increase the risks of osteoporosis and future fracture. Maintaining a bone healthy lifestyle at all ages (Table 4.1) is an important part of mitigating the expected increase in osteoporosis and fracture in all countries, but is most important where change is likely to be greatest.
Table 4.1 Bone healthy lifestyle
Adequate dietary calcium
Adequate vitamin D through diet and sunlight exposure
Regular weight bearing exercise
Avoid smoking
Avoid excess alcohol
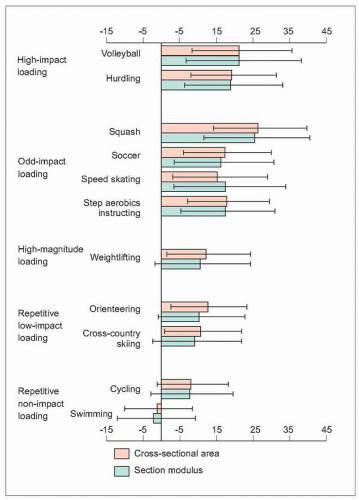
4.1 High impact exercises are associated with the greatest effect on the bone structure as measured by cross-sectional area and section modulus. (Adapted from Nikander R, et al. (2005). Femoral neck structure in adult female athletes subjected to different loading modalities. J Bone Min Res20:520-528.)
Physical activity and exercise
Maintaining a strong skeleton at all ages relies on mechanical stimuli from weight bearing and physical activity. The risk of falling is reduced by maintaining physical fitness. Risk of fracture is increased in those physically inactive; walking for 4 hours a week was found to be associated with a 41% lower risk of hip fracture in postmenopausal women aged 40-77 years1. Immobility, such as bed rest, rapidly causes bone loss that can only be slowly regained. People are, however, becoming less physically active and fit in all countries and cultures. It is estimated that 17% of adults in the world are physically inactive and only an average of 41% of adults are doing some, but insufficient physical activity (<2.5 hours per week of moderate activity)2. Physical activity declines with ageing.
Physical activity increases bone mass, density, quality, and strength. The benefit of physical activity is greatest at or before puberty3. The response of the skeleton in adulthood to physical activity is less but maintenance of, or increases in, bone density has been demonstrated with impact and nonimpact exercise regimes in pre- and postmenopausal women4,5,6. A greater benefit is seen in those with high calcium intake7. The effect of exercise is site specific, benefiting most the loaded site, but the characteristics of the exercise that is most effective is not clear. Impact type sports are probably best at improving bone strength, such as tennis, aerobics, basketball, gymnastics, or weight training (4.1), and for older people brisk walking and using stairs are probably of benefit. The frequency and duration required are unclear. The long-term benefits are uncertain; in some studies stopping exercise has shown that the bone density returns to baseline levels8. Whether the improvements in bone density translate into a reduction in fracture risk is not yet established.
Although physical exercise programs may only increase bone mass by a marginal percent, the additional benefits from improved gait, balance, coordination, and muscle strength contribute to a potential antifracture effect. Poor balance and quadriceps weakness are predictors of falls and fracture. Programmes of muscle strengthening and balance retraining, individually prescribed by a trained health professional and Tai Chi exercises are likely to prevent falls in elderly people9, but there is little evidence for other forms of exercise. Although these measures may prevent falls, there is little evidence that this results in prevention of fractures. Epidemiological studies do, however, show that past and present physical activity does relate dose dependently to risk of hip fracture.
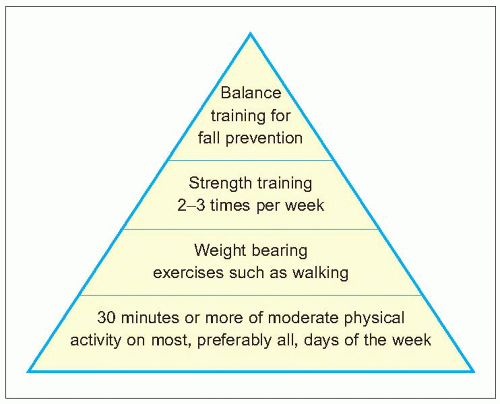
From these studies it is recommended to be physically active at all stages of life, with vigorous activities in early years and moderate activity in older life such as regular brisk walking of at least 30 minutes daily (4.2). Greatest benefits are during growth and development, and establishing lifelong exercise habits will have long-term benefit. Those who are less active, especially the sedentary elderly, will also benefit from increasing their level of physical activity. To be effective, physical activity should be weight bearing, easy, enjoyable, sociable, and fit into everyday routines so that it is sustainable throughout life. There are also other health benefits of increasing physical fitness such as reducing the risk of heart disease. The utility of a formal exercise intervention beyond this in maintaining or increasing bone mass and reducing fractures in later life in the general population is problematic, as long-term sustainability is necessary for real benefits and the best way to influence such behaviour is not clear10.
Diet, nutrition, and body weight
Body weight and nutrition are important determinant of bone mineral density (BMD) and risk of fracture and their outcome. They are important at all stages of life. Bone density is closely related to body weight11 in men and women across all ages and throughout the skeleton. Changes in bone density also relate to body weight: the risk of hip fracture is greater with low body weight and with weight loss12,13. Women who were relatively thin when 50-64 years and had lost at least 10% of their body weight had the highest risk of hip fracture12. The fracture risk is in part related to osteoporosis and bone strength, but also to less protective soft tissue. Anorexia nervosa can be associated with severe osteoporosis and premature occurrence of fractures (see 2.41), which is a consequence of poor nutrition, low body weight, and sex hormone deficiency.
Normal nutrition is important for the development and maintenance of the skeleton (Table 4.2). Undernutrition is associated with a reduced peak bone mass and acceleration of age-related bone loss14,15. People with hip fracture are often under- or malnourished. Undernutrition may increase the propensity to falls, possibly a consequence of impaired coordination and reduced muscle strength. The consequences of falls are worse due to less protective soft tissue, and the outcome following fracture is worse with prolonged hospital stays, more complications, and increased mortality. Undernutrition increases with advancing age and may relate to the spontaneous reduction of food intake, to malabsorption, or to intercurrent illnesses. Protein-calorie malnutrition is the most common problem in the elderly but there are also deficiencies in micronutrients such as calcium and vitamin D (see below). Low intakes of vitamin K may also increase the risk of hip fracture in women. Low body weight and undernutrition are also associated with comorbidity and general frailty in an ageing population, all of which will increase the risk of fracture and worsen the outcome.
4.2 General recommendations for physical activity in adults. (Adapted from U.S. Department of Health and Human Services (2004). Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville MD: Department of Health and Human Services, Office of the Surgeon General.)
Ensuring adequate nutrition with a balanced diet to provide the needed macro- and micronutrients and that will maintain an ideal body weight is therefore recommended16 (Table 4.3). Although energy requirements decrease with advancing age, the recommended dietary allowance of protein increases from 0.8 g/kg of body weight in young adults to 1 g/kg in the healthy elderly. Protein supplementation in patients with recent hip fracture has been shown to improve the clinical outcome with reduction in complications, shorter hospital stays, and reduced subsequent bone loss14,15. Dietary protein intake has also been shown to be associated with a reduced risk of hip fracture in men and women aged 50-69 years17. The role of other nutritional supplements is not clear. Phytoestrogens are plant products with some oestrogen-like structures and actions including the potential to act on bone. They may have a role in preventing osteoporosis and fracture but there is presently a lack of data on efficacy.
Smoking
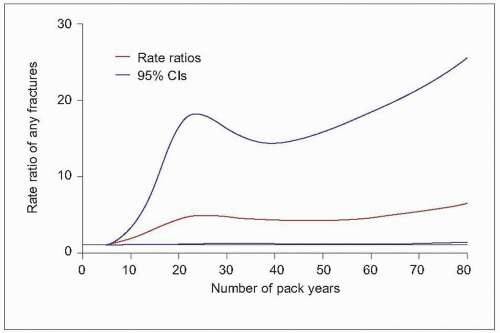
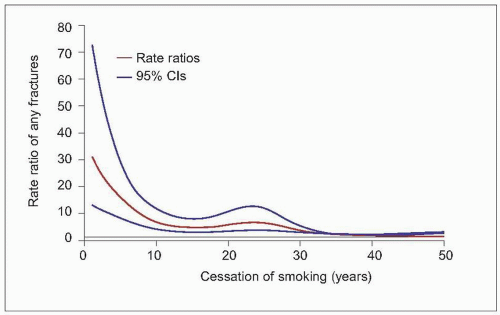
Smoking carries a moderate and dose-dependent risk for osteoporosis and fracture18,19,20. In a longitudinal populationbased cohort study of men first enrolled at 50 years and followed for 27 years, the risk of any fracture increased linearly with smoking up to about 25 pack-years. At higher rates of consumption there was no further substantial increase in fracture risk per pack-year (4.3)21. Reduced bone mass has been shown in different populations around the globe22 at all sites, most marked at the hip23. This will increase the risk of fracture; it is estimated that smoking increases the lifetime risk of hip fracture by 31% in women and 40% in men23. The increased risk of fracture has been demonstrated at all sites in both men and women, and is greatest for hip fracture, with estimates of a relative risk of 1.84 (95% CI 1.52-2.22). This increased risk is not only explained by effects on bone density and body mass index (BMI)20. Past smokers are at intermediate risk19 and it would, therefore, appear that stopping smoking will reduce the risk of osteoporosis and fracture. However, the benefit may not be seen for 10 years in women24 but could be up to 30 years in men21 (4.4).
Table 4.2 Nutrition and bone
Undernutrition in older persons:
Spontaneous reduction in food intake
Malabsorption
Intercurrent illness
Protein-calorie malnutrition most common problem
Effects of undernutrition:
Reduced peak bone mass
Accelerated age-dependent bone loss
Hip fracture cases are often under- or malnourished
Increased risk of falling
Impaired coordination
Reduced muscle strength
Consequences of falls worse due to less protective soft tissues
Outcome of fracture worse with increased morbidity and mortality
Table 4.3 Nutrients of importance for bone health
Convincing evidence of association with decreased risk of osteoporotic fracture:
Calcium
Vitamin D
Possible association with decreased risk of osteoporotic fracture:
Protein
Phytoestrogens
Fruits and vegetables
Plausible association with decreased risk of osteoporotic fracture:
Zinc
Copper
Manganese
Boron
Vitamin A
Vitamin C
Vitamin K
B vitamins
Potassium
Sodium
(Adapted from: WHO (2003). Diet, nutrition and the prevention of chronic diseases. WHO Technical Report Series No. 916. World Health Organization, Geneva.)
4.3 Risk of fracture associated with smoking in a longitudinal population-based cohort study of men. (Adapted from Olofsson H, et al. (2005). Smoking and the risk of fracture in older men. J Bone Min Res20:1208-1215.)
4.4 Risk of fracture following smoking cessation in a longitudinal populationbased cohort study of men. (Adapted from Olofsson H, et al. (2005). Smoking and the risk of fracture in older men J Bone Min Res20:1208-1215.)
Alcohol
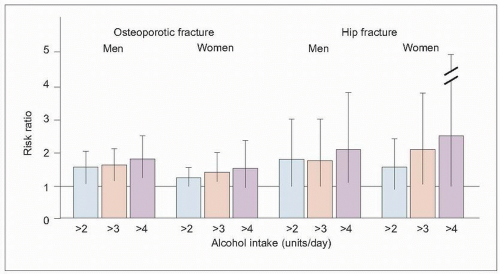
Alcohol affects bone metabolism, whether acute or chronic consumption, moderate or excessive. Chronic alcohol abuse is associated with osteoporosis and fracture, and is a common cause of secondary osteoporosis in men. An increase in osteoporotic (RR 1.38, 95% CI 1.16-1.65) and hip fractures (RR 1.68, 95% CI 1.19-2.336) was found in an analysis of several large population studies25. The risk of fracture increases with alcohol intake above a threshold of 2 units daily in both men and women in a study of three prospective cohorts of 5,939 men and 11,032 women in total, followed for a total of over 75,000 person-years25 (4.5). The effect was nonlinear and seen above an intake of 3 units daily in both men and women.
The effect of chronic heavy drinking on the skeleton during adolescence and young adulthood is particularly harmful leading to future osteoporosis (see 2.42). The effect is increased because of other frequently coexistent lifestyle risk factors such as smoking, poor diet, and lack of physical activity. People who drink alcohol are more likely to smoke than nondrinkers, and smokers are much more likely to drink than nonsmokers. Eating disorders are common in women who abuse alcohol. The risk of fracture may relate to an increased risk of falls with greater physical impact, in addition to reduced BMD. Moderate alcohol consumption, in contrast, may not be harmful25,26 and may even be beneficial with increased bone density, but it does not seem to reduce fracture risk. There is little evidence as to the effect of reducing alcohol intake; in the Framingham Study27 there was no effect on fracture risk of changing from a past heavy to a present light alcohol intake, but avoidance of excess is recommended (which has additional health benefits).
Calcium and vitamin D
Many studies have examined the role of adequate dietary calcium and vitamin D in maximizing bone density and preventing fracture. These have looked at the role of calcium and vitamin D in bone health from an epidemiological perspective, using dietary changes or by the use of supplements in people unselected for their calcium and vitamin D status, or in people known or likely to be deficient. The interest in these dietary constituents is because calcium is the basic requirement for bone mineralization and is needed for the normal development and maintenance of the skeleton, and because of the known role of vitamin D in bone metabolism (see Chapter 1 and see below).
4.5 Risk of fracture with alcohol intake. (Kanis JA, et al. (2005). Alcohol intake as a risk factor for fracture. Osteopor Int16:737-742).
Serum calcium levels are tightly regulated as calcium is essential for transmembrane transportation and cell communication for all cell types throughout the body. Bone tissue is the main calcium reservoir, and the bone mineral content is regulated through feedback systems that involve parathyroid hormone (PTH), calcium, and vitamin D. PTH initiates bone resorption in response to low levels of calcium. Consequently, insufficient calcium intake or absorption to offset the obligatory losses in the urine, digestive juices, and sweat may provoke a continuous upregulation of PTH release, causing increased bone loss. This low-grade secondary hyperparathyroidism is not uncommon in the elderly. This mechanism provides the rationale for calcium and vitamin D treatment as part of a strategy to prevent bone loss, particularly in the elderly.
Adequate calcium intake is important in achieving optimal peak bone mass and an increased calcium intake is of benefit if the baseline dietary calcium intake is low. In later life, low calcium intake is associated with an increased risk of fracture28, including in Asian men and women29. Dietary calcium intake declines with ageing and many people consume less than the recommended daily allowance. In addition, there is a decline in efficiency of calcium absorption with ageing.
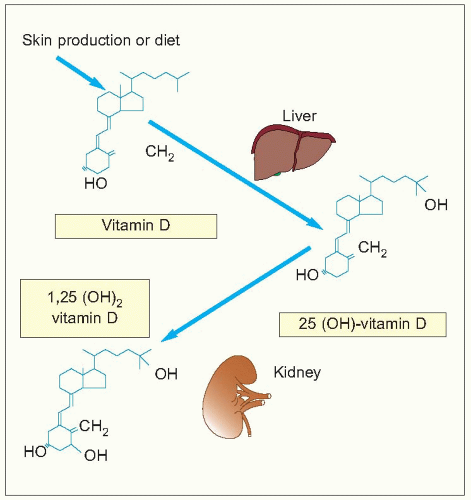
Vitamin D plays a central role in calcium regulation. It is either provided through the food intake or by exposure of the skin to sunlight. Vitamin D, in the ingested form or from dermal conversion of 7-dehydrocholesterol by ultraviolet light, is biologically inactive until metabolized through several steps in the liver and kidneys (4.6). Vitamin D insufficiency is common in the elderly, particularly in northern latitude countries with few hours of sunlight. Skin synthesis is less efficient due to an age-related decline in the amount of 7-dehydrocholesterol (a precursor of vitamin D) in the epidermal layer of the skin, along with older people spending less time outdoors in sunlight. Many older people who are osteoporotic or sustain fractures have low levels of vitamin D. This may not only be relevant to reduced bone strength but there may also be muscle weakness as a consequence, with increased risk of fracture. It is therefore apparent that inadequate calcium and vitamin D are deleterious to bone health but the evidence for the benefit of supplementation to correct this is less clear.
Calcium
The effectiveness of calcium supplementation in the prevention and treatment of osteoporosis remains under debate, particularly concerning fracture as outcome. Studies using calcium supplement alone have shown conflicting results. In a recent meta-analysis that included 15 studies and a total of 1806 postmenopausal women, a small but significant effect on bone density was seen at all measured sites30. The antifracture effect was estimated at a relative risk of 0.77 (95% CI 0.54-1.09) for vertebral fractures and 0.86 (95% CI 0.43-1.72) for nonvertebral fractures, and was not significant because of a too small sample size. Benefits are greatest in those with a low calcium intake31. In almost all randomized controlled trials (RCTs) for bone specific antiresorptive agents, calcium supplementation (400-800 mg) is included in the placebo group that show a 0.5-2 % gain in bone mass.
4.6 Metabolic pathway of vitamin D.
Vitamin D
Vitamin D3 supplements alone, usually 400 IU/day with the assumption of an adequate dietary calcium intake, have not been shown to reduce the incidence of fractures in studies of elderly men and women living in the community32 or in nursing homes33. A recent Cochrane review34 showed no significant effect on hip fracture (seven trials, 18,668 participants), vertebral fracture (four trials, 5698 participants), or any new fracture (eight trials, 18,935 participants).
Vitamin D has, nevertheless, been shown to reduce the risk of fracture in community living men and women given as 100,000 IU oral cholecalciferol every 4 months over 5 years35. Vitamin D has also been shown to increase femoral neck bone density (0.2-2.6%) or reduce the rate of loss in elderly women after 2 years of treatment, while other skeletal sites remain similar compared to the placebo groups36,37. The dose required to obtain a measurable bone effect over this period was between 400-800 IU/day.
Vitamin D has also been shown to reduce the risk of falls among ambulatory or institutionalized older people by over 20% in a meta-analysis of 5 RCTs including 1237 participants38. This effect of vitamin D may explain some of the benefit in studies of calcium combined with vitamin D.
Calcium combined with vitamin D
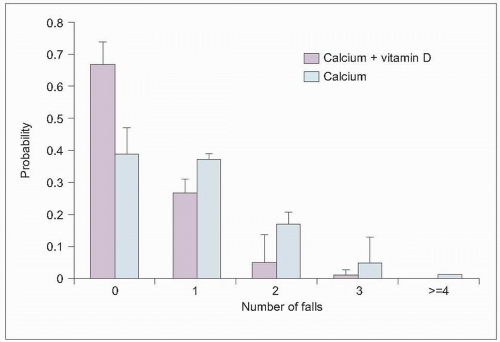
Calcium and vitamin D in combination is the accepted baseline treatment for osteoporosis and also as a preventive measure, in particular in the frail elderly. Calcium and vitamin D supplementation (1200 mg calcium and 800 IU vitamin D) over 12 weeks in elderly women reduced the risk of falling39 (4.7). This has been confirmed in a metaanalysis38. Recent studies have, however, made it less clear as to whether groups other than the frail elderly will benefit.
In a large RCT of elderly French nursing home patients with calcium (1200 mg) and vitamin D (20 μg [800 IU]) there was significant reduction in new hip (RR 0.70 [95% CI 0.62-0.78]) and for all nonvertebral fractures (RR 0.70 [95% CI 0.51-0.91]) after 3 years of treatment, with significant benefit at 18 months40,41 (Table 4.4).
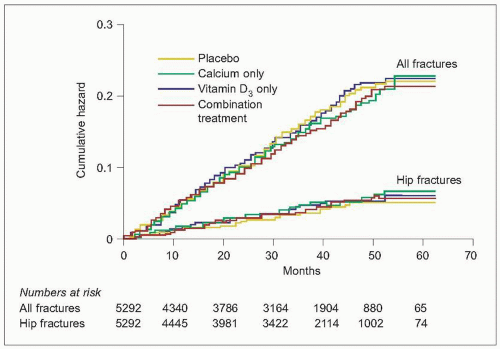
Several recent studies have examined further the effectiveness of calcium and vitamin D in combination. In a large pragmatic RCT in the secondary prevention of osteoporotic fractures42, 4,481 women and 811 men aged 70 years and over who had sustained a low trauma fracture were randomized to receive (1) 1000 mg calcium daily, (2) vitamin D 800 IU daily, (3) calcium (1000 mg) in combination with vitamin D (800 IU), (4) placebo. The parti cipants were ambulatory and mostly community dwelling. During between 24 months and 62 months follow-up, 13% sustained a new low-trauma fracture, one-quarter of which were of the hip; there was no difference in the incidence of fractures in the three treatment groups (4.8). The vitamin D status was only measured in a small sample and compliance with treatment was two-thirds or less at 2 years.
4.7 Effects of calcium and vitamin D supplementation on the risk of falling. (Adapted from Bischoff HA, et al. (2003). Effects of vitamin D and calcium supplementation on falls: a randomized controlled trial. J Bone Min Res18:1342-1343.).
Another large pragmatic open RCT of women aged 70 years and over with risk factors for hip fracture failed to find evidence that supplementation with 1000 mg calcium and 800 IU vitamin D daily over a median follow-up of 25 months reduces the risk of fracture or falls43. A total of 3314 patients were included in the study and 1321 were randomized to treatment; the 1993 controls were just given advice on prevention of falls and osteoporosis. At 12 months follow-up, only 63% of the intervention group was adhering to treatment. Vitamin D status of participants was not established either before or during the study.
The recent Cochrane review34 of seven trials and 10,376 participants, including those studies detailed above, found a small reduction in hip fractures (RR 0.81, 95% CI 0.68-0.96) and nonvertebral fractures (RR 0.87, 95% CI 0.78-0.97). Most recently, the Women’s Health Initiative study of more than 36,000 postmenopausal women aged 50-79 years randomly assigned to 1000 mg calcium and 400 IU vitamin D daily or placebo for an average of 7 years has failed to show any reduction in fractures unless just those adhering to treatment were included44.
It appears that the vitamin D status of the person and their level of independence makes a difference in response to calcium and vitamin D. It is, however, unfortunate that vitamin D levels were not measured comprehensively in recent studies to help clarify who will benefit most. Effectiveness in clinical practice is also reduced by lack of long-term adherence to treatment. The role of calcium and vitamin D supplements therefore remains unresolved, but it is reasonable to ensure that deficiency is avoided at all stages of life, in particular in the growing skeleton and in the frail elderly. It is easier to achieve sufficiency through dietary intake and sunlight exposure when exercising in younger people but supplements may be needed in the frail elderly. The role of supplementation in those who are mobile with reasonable diets and sunlight exposure, even if elderly, is not proven.
Table 4.4 Calcium and vitamin supplementation in a very elderly population in care
Vitamin D + calcium
Placebo
Pvalue
Active treatment analysis
Number of women
872
893
Hip fracture ≥1
109
153
<0.01
Nonvertebral fractures ≥1
205
270
<0.01
Intention to treat analysis
Number of women
1176
1127
Hip fractures ≥1
137
178
<0.02
Nonvertebral fractures ≥1
255
308
<0.02
(Adapted from Chapuy MC, et al. (1994). Effect of calcium and cholecalciferol treatment for three years on hip fractures in elderly women. BMJ308:1081-1082.)
4.8 Effects of calcium, vitamin D, or combination treatment on the incidence of new low-trauma fracture. (Adapted from Grant AM, et al. (2005). Oral vitamin D3 and calcium for secondary prevention of low-trauma fractures in elderly people (Randomized Evaluation of Calcium Or vitamin D, RECORD): a randomized placebo-controlled trial. Lancet365(9471):21-1628.)
Recommended supplementation if being used is:
Calcium 500-1000 mg depending on dietary intake to reach above a total of 1000 mg/day.
Vitamin D 400-800 IU daily – the higher dose may be indicated for institutionalized persons or those receiving equivalent care, or during the winter in northern latitude countries.
A bone healthy lifestyle
There are several potentially modifiable risk lifestyle factors associated with reduced bone density and increased risk of fracture (see above). It has been estimated that if the whole population undertook and achieved a high level of physical activity and calcium consumption that the population risk of hip fractures could be reduced by about 17% in older women45, and avoiding undernutrition, smoking, and excess alcohol would have greater benefits (4.9); the challenge is achieving such changes in peoples behaviour.
4.9 A bone healthy lifestyle.
Table 4.5 Categories of evidence
Ia
Evidence from meta-analysis of randomized controlled trials
Ib
Evidence from at least one randomized controlled trial
IIa
Evidence from at least one controlled study without randomization
IIb
Evidence from at least one other type of quasi-experimental study
III
Evidence from descriptive studies, such as comparative studies, correlation studies and case-control studies
IV
Evidence from expert committee reports or opinions or clinical experience of respected authorities, or both
(Adapted from Eccles M, et al. (1998). North of England evidence based guidelines development project: methods of developing guidelines for efficient drug use in primary care. BMJ, 316(7139):1232-1235.)
PHARMACOLOGICAL INTERVENTIONS
Pharmacological interventions in osteoporosis rely on targeting osteoclasts, osteoblasts, or both. The rationale for inhibition of osteoclasts stems from a number of observations; most important was the observation that oestrogen withdrawal led to increased osteoclast activation and hence blocking osteoclast differentiation and actions seemed essential. Inhibition of osteoclast action leads to a secondary gain in bone mass. In addition, it has clearly been more difficult to stimulate osteoblasts selectively to obtain a true bone anabolic effect. An ideal bone agent should have a dual effect and preferably increase not only bone mass but also improve bone quality and strength.
Bone turnover is a slow process and, as a consequence, evaluation of treatment effect in terms of bone gain and fracture reduction is extended over time, i.e. 1-3 years. This has an impact on design of trials and outcome evaluation. From an evidence-based perspective, fracture efficacy should be the primary end-point of all studies; however, if fracture efficacy is proven (Table 4.5), change in BMD and change in bone markers may serve as surrogate end-points, albeit recognizing the limitations of this approach.
Evidence of effect on fracture is the required end-point for any osteoporosis treatment to be considered of clinical value. The strength of evidence depends on the source. The best evidence is considered to be from the meta-analysis of several RCTs, whereas the weakest evidence is considered to be unsupported expert opinion. Recommendation of treatment should be based on evaluation using these established criteria for evidence of efficacy. This approach is used in guideline development46.
Bisphosphonates
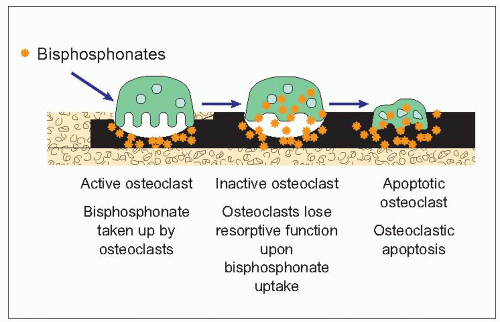
Bisphosphonates are chemically developed from pyrophosphates, compounds that inhibit precipitation of calcium carbonate and have industrial applications. Bisphosphonates act by binding to the mineral phase of bone, binding to hydroxyapatite. Osteoclast activity is reduced with decreased ruffle border, decreased acid production, and decreased production of lysosomal enzymes and prostaglandins (4.10). Osteoclast numbers are reduced by increased apoptosis and inhibition of osteoclast recruitment. They have little effect on other organ systems. Bisphosphonates are known to markedly suppress bone turnover. It has been estimated that bone resorption must be suppressed by 40-80% in order to obtain a significant effect on BMD. Since bisphosphonates primarily affect the activity of osteoclasts, the effects on bone resorption markers have gained most interest.
Bisphosphonates are, in general, poorly absorbed from the gastrointestinal tract. Only about 0.5-5% of a given dose is absorbed from the stomach, further decreased by food intake (particularly calcium-containing foods) or even drinks such as coffee or juice. Oral bisphosphonates must, therefore, be taken after a food-free interval of an overnight fast and a fast of 30-60 minutes after taking them. The possibilities of less frequent dosing with highly potent oral compounds, as well as the development of intravenous administration are therefore much more convenient from the persons’ viewpoint and potentially more effective due to better adherence to therapy. About half of the absorbed drug is excreted unmetabolized in the urine. Bisphosphonates are deposited in bone for a prolonged time, probably up to 10 years or more47.
4.10 Bisphosphonate mechanism of action.
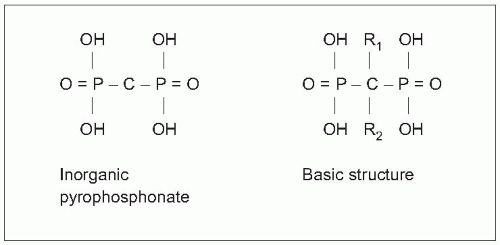
A core P-O-P bond, which in bisphosphonates is exchanged with a P-C-P bond, characterizes the basic pyrophosphate structure. This allows for two side chains (R1 and R2), with R1 binding to hydroxyapatite and R2 giving the specific biological and chemical properties (4.11, 4.12). The potency of each bisphosphonate compound depends on side chain substitution. Nitrogen-containing bisphosphonates are most potent and exert their inhibitory effect through the mevalonate pathway. This allows for lower doses and less frequent dosing.
Alendronate
Alendronate, a second generation bisphosphonate, was the first bisphosphonate for which a clear antifracture effect was seen in RCTs.
Effect on bone turnover
Alendronate suppresses bone turnover within 6-12 weeks48 (4.13). The effect is most pronounced for bone resorption markers, decreasing 40-60% and results in a sustained increase in bone density in the axial and appendicular skeleton49 (4.14).
Effect on BMD
The first study, which included postmenopausal women with low bone density (T-score < -2.5) with or without prevalent vertebral deformity, showed BMD increases of 8.8% and 5.9% in the spine and hip, respectively. The effect, including reduction in new vertebral fractures was most pronounced in women above age 65 and with at least one vertebral fracture at entry.
4.11 Basic structure of bisphosphonate.
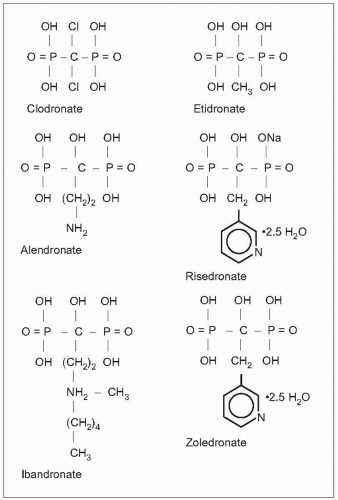
4.12 Structure of clodronate, etidronate, alendronate, risedronate, ibandronate and zoledronate.
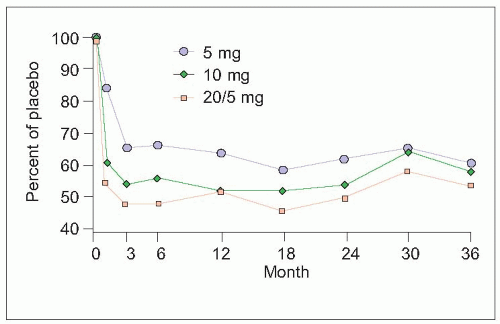
4.13 The effect of alendronate on bone markers. (Adapted from Devogelaer JP, et al. (1996). Oral alendronate induces progressive increases in bone mass of the spine, hip, and total body over 3 years in postmenopausal women with osteoporosis. Bone, 18(2):141-150.)
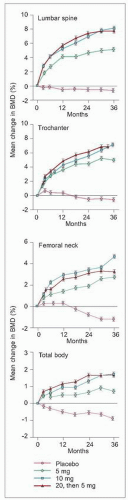
4.14 The effect of alendronate on BMD. (Adapted from Liberman UA, et al. (1995). Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. The Alendronate Phase III Osteoporosis Treatment Study Group. N Engl J Med,333(22):1437-1443.)
Effect on fracture
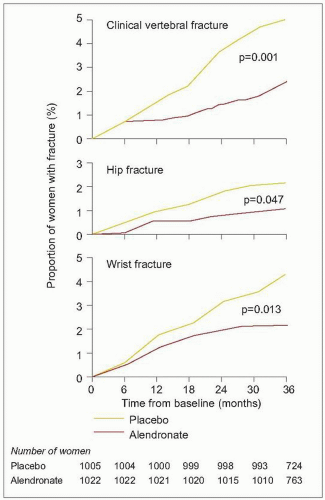
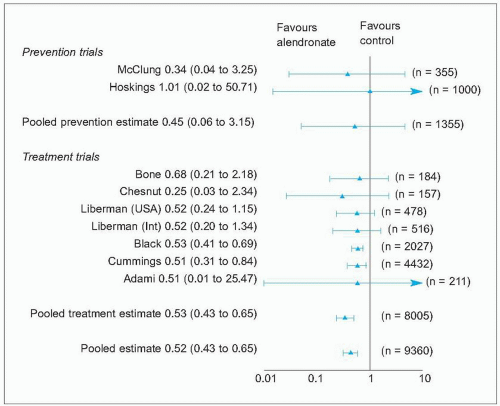
Two major trials49, 50 have shown a reduction in vertebral deformities of about 50%, and prevention of nonvertebral fractures has been demonstrated (4.15). In the Fracture Intervention Trial 1 (FIT 1), 2027 women with at least one prevalent vertebral fracture were included. Alendronate treatment over 3 years gave a clear reduction in the number of new radiographic and clinical vertebral fractures (p=0.001) and also a reduction of hip (p=0.047) and wrist fractures (p=0.013), albeit the number of fractures was small. In a meta-analysis of 11 RCTs with alendronate, pooled data favours an antifracture effect from alendronate treatment with 5 mg or greater, with a risk reduction of 47%. Reduction of nonvertebral fractures is also evident in postemenopausal women fulfilling the criteria for osteoporosis51 (4.16).
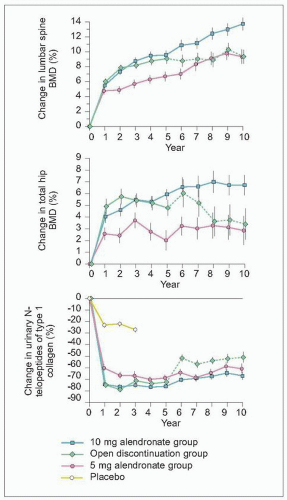
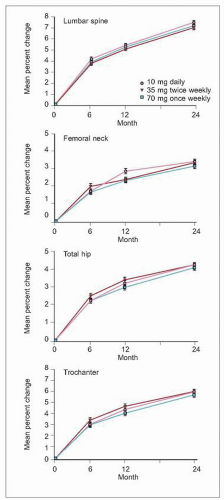
The effect of alendronate has been shown to be sustained long term52 (4.17). It has been possible to monitor long-term effects of alendronate treatment in a subset of women from some of the early studies. Thus, 10-year treatment effects are reported in 247 women (4.18)53. The increase in BMD is maintained with an even further increase in spinal BMD (13.7%). Similarly, bone markers stayed depressed. In those discontinuing treatment, the BMD gain remained in the spine, whereas a decrease was obvious in the hip. The BMD effect of 10 mg daily, 35 mg twice weekly, and 70 mg once weekly of alendronate is similar over 2 years in women with postmenopausal osteoporosis (4.19). The preferred dosing regimen is now 70 mg once weekly54, 55.
Risedronate
Risedronate is a third generation, highly potent bisphosphonate that has also been shown to prevent vertebral and nonvertebral fractures. Risedronate is a nitrogen-containing bisphosphonate that, like other nitrogen-containing bisphosphonates, is likely to induce apoptosis through inhibition of farnesyl or geranylgeranyl isoprenoid groups through the mevalonate pathway56.
Effect on bone turnover
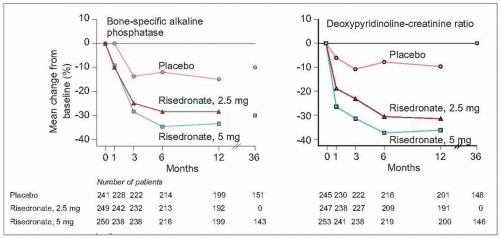
A major 3-year RCT evaluating the antifracture efficacy of risedronate included 2458 postmenopausal women in North America with prevalent vertebral deformities57. In this study of risedronate, deoxypyridinoline was dose-dependently suppressed by about 40%, an effect that was evident within 1 month of risedronate treatment (4.20, left). The secondary effect on bone formation, as measured by bonespecific alkaline phosphatase was delayed, reaching a maximum depression at 3-6 months (4.20, right). The effect is less pronounced than that of alendronate, which can be interpreted either as a positive or negative outcome; negatively as it indicates a lower efficacy or positively as adverse effects on mineralization from marked long-terms suppression is less likely.
Effect on BMD
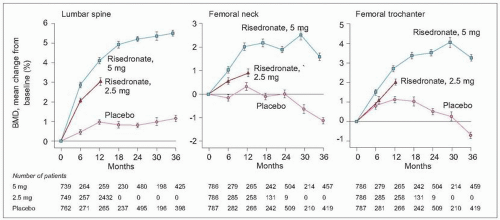
The effect of risedronate on bone density is similar to that of alendronate, producing about 4-6% increase in spinal and femoral bone mass after 3 years of treatment. The dosedependent effect of risedronate evident from bone marker assessment is associated with a similar effect on BMD (4.21). Hence, the 2.5 mg/day dose was discontinued within the study, whereas a significant increase in BMD was found for the 5 mg dose. BMD increase was most pronounced in the lumbar spine (5.4%), with a 1.6% increase in the femoral neck and 3.3% in the trochanteric region compared to placebo.
4.15 The effect of alendronate on fracture. (Adapted from Black DM, et al. (1996). Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet,348(9041):1535-1541.)
4.16 Alendronate metaanalysis. (Adapted from Cranney A, et al. (2002). Meta-analyses of therapies for postmenopausal osteoporosis. II. Metaanalysis of alendronate for the treatment of postmenopausal women. Endocr Rev, 23(4):508-516.)
4.17 Alendronate 7-year data. (Adapted from Tonino RP, et al. (2000). Skeletal benefits of alendronate: 7-year treatment of postmenopausal osteoporotic women. Phase III Osteoporosis Treatment Study Group. J Clin Endocrinol Metab, 85(9):3109-3115.)
4.18 Alendronate 10-year data. (Adapted from Bone HG, et al. (2004). Ten years’ experience with alendronate for osteoporosis in postmenopausal women. N Engl J Med, 350(12):1189 -1199.)
4.19 Alendronate and dosing. (Adapted from Rizzoli R, et al. (2002). Two-year results of once-weekly administration of alendronate 70 mg for the treatment of postmenopausal osteoporosis. J Bone Miner Res17(11):1988-1996.)
Effect on fracture
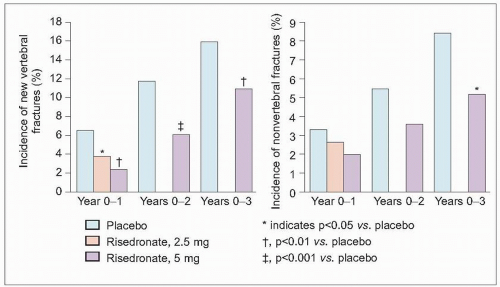
The antifracture effect on vertebral fracture was evident after 1 year of treatment and sustained at 3 years, with a 41% cumulative decrease in radiographic vertebral fracture incidence (defined as more than 15% loss of vertebral height). Nonvertebral fractures were significantly lower (39%) at 3 years compared to placebo (4.22).
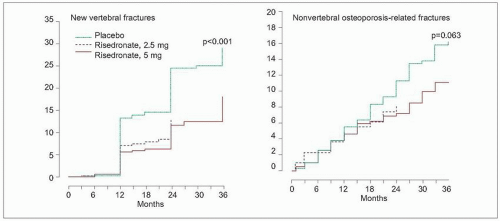
The results of the study was to some extent hampered by a rather high discontinuation rate (up to 45%) for various reasons. However, the results of the European and Australian arms of the trial (n=1226) indicates similar effects: vertebral fractures were reduced by 49% in those treated with 5 mg per day. The effect was evident after the first year. Nonvertebral fractures were reduced by 33%; however, this was not significant (p=0.06) (4.23)58.
4.20 Risedronate and effect on bone markers. (Adapted from Harris ST, et al. (1999). Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial.
Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA, 282(14):1344-1352.)
4.21 Risedronate effect on BMD. (Adapted from Harris ST, et al. (1999). Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA,282(14):1344-1352.)
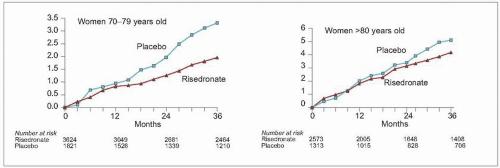
Hip fracture is the most devastating fracture for the individual with substantial subsequent morbidity and mortality. The effect of risedronate on hip fracture risk was specifically evaluated in a high-risk population of 5445 women aged 70-79 years and in 3886 women aged 80 and above (4.24). Women were included based on BMD measurement and/or on risk factors. In women aged 70-79 years with osteoporosis, the incidence of hip fracture was reduced by 40% (RR 0.6, 95% CI 0.4-0.9). In women aged 80 and above, included primarily based on risk factors, there was no fracture-sparing effect59. Again this study points out that low bone density is a major determinant for the clinical effect of antiresorptive agents.
4.22 Risedronate effect on fracture. (Adapted from Harris ST, et al. ( 1999). Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA,282(14):1344-1352.)
4.23 Risedronate effect on fracture. (Adapted from Reginster JY, et al. (2000), Randomised trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Osteoporos Int, 11:83-91.)
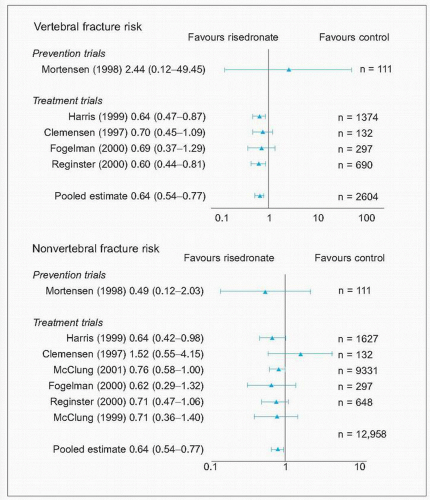
In a meta-analysis, including eight RCTs fulfilling the inclusion criteria of the analysis, fracture risk for vertebral fractures was reduced by 36% in doses of risedronate above 2.5 mg per day (RR 0.64, 95% CI 0.54-0.77) (4.25). The comparable risk reduction for nonvertebral fractures were 27% (RR 0.73, 95% CI 0.61-0.87)62. Meta-analyses is the highest level of evidence for a treatment effect, thus it can be concluded that risedronate substantially reduces the risk of both vertebral and nonvertebral fractures.
4.24 Risedronate effect on hip fracture. (Adapted from McClung MR, et al. (2001). Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med, 344(5):333-340.)
4.25 Risedronate meta-analysis – vertebral fracture risk and nonvertebral fracture risk. (Adapted from Cranney A, et al. (2002). Meta-analyses of therapies for postmenopausal osteoporosis. III. Meta-analysis of risedronate for the treatment of postmenopausal osteoporosis. Endocr Rev,23(4):517-523.)
Safety
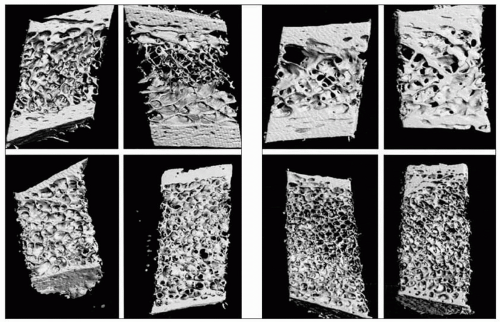
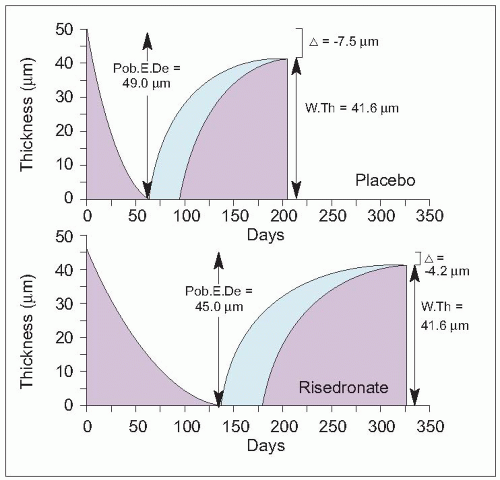
Since bisphosphonates are incorporated into the mineralized matrix very long term (up to 10 years), adverse effects from long-term suppression of bone turnover have been a concern. In one study, pretreatment transiliac bone biopsies were compared with biopsies taken after 3 years of risedronate treatment (4.26)60. Histomorphometric evaluation indicated, as expected, a moderate effect on bone turnover with a 47% decrease in activation frequency. The study did not observe any structural alteration in treated women compared to nontreated women. In an additional study, it has been estimated that changes in lumbar spine BMD only explains 18% of the vertebral fracture efficacy, which may be interpreted as that other qualitative traits may also contribute to fracture risk61. In order to further evaluate qualitative traits three-dimensional microcomputed tomography was performed in bone biopsies from treated and nontreated women. In those on placebo, microstructural architecture deteriorated, with for example a 13% increase in trabecular separation, in contrast to those treated with risedronate (4.27).
The effect of risedronate treatment has been evaluated up to 7 years in the multinational arm of the Fracture Study58. Of the initial study cohort, 164 women were available for the extension study and, after additional randomization, were treated with placebo or risedronate. In those treated with risedronate for 7 years, bone turnover was consistently decreased and BMD remained significantly increased with about 4% increase in the hip and 8-11% in the spine63. Weekly dosing of risedronate gives similar changes in bone markers and a similar BMD response and is the preferred regimen for the purpose of adherence64. Risedronate has also been used in men, with similar effects on bone mass and with a significant reduction of vertebral fractures65.
4.26 Effects of long-term risedronate on bone quality and bone turnover in women with postmenopausal osteoporosis. (Adapted from Eriksen EF, et al. (2002). Effects of long-term risedronate on bone quality and bone turnover in women with postmenopausal osteoporosis. Bone, 31(5):620-625.)
4.27 Risendronate and effect on bone quality. (From Dufresne TE, et al. (2003). Risedronate preserves bone architecture in early postmenopausal women in 1 year as measured by three-dimensional microcomputed tomography. Calcif Tissue Int73(5):423-432 with permission.)
Side-effects
Risedronate, as other bisphosphonates, must be taken according to instructions. It appears to be well tolerated both in the studies and clinically, with no serious side-effects reported. Since negative gastrointestinal effects have been a concern, the gastroduodenal effects have been specifically evaluated in comparison to alendronate and found to be significantly lower66. From an observational cohort study conducted using the UK GP database of over 13,000 patients, ophthamological side-effects were specifically evaluated and occurred in a small proportion of the patients (n=313)67. This indicates that a number of different sideeffects may occur but these are usually mild.
Ibandronate
Ibandronate is a new addition to the nitrogen-containing bisphosphonates for the treatment of osteoporosis. In general, ibandronate has similar properties to other nitrogencontaining bisphosphonates, but is 2-, 10-, and 50-fold more potent than risedronate, alendronate and pamidronate, respectively68. Bisphosphonates are poorly absorbed after oral administration, with 0.5-1% absorption when taken according to instructions after an overnight fast and at least 30 minutes before breakfast. For ibandronate this means that efficacy drops and is 100-fold less with oral administration. Hence, ibandronate is suitable for intravenous administration, but based on the high potency, the dosing interval after oral administration can also be increased. Weekly dosing of other bisphosphonates has been available for some time, but from studies it is evident that women would prefer even longer dosing interval as it would fit better with their lifestyle69. Similarly, in a comparative study oncemonthly ibandronate was preferred over once-weekly alendronate in a cross-over trail70. The availability of highpotency bisphosphonates such as ibandronate has promoted development of dosing regimens with extended drug free periods using both intravenous and oral administration. It needs to be borne in mind, however, that the potency in experimental models does not necessarily transfer to a similar difference in potency in clinical effect in patients.
Ibandronate is described as a third generation bisphosphonates with a hydroxyl group at R1 chain and a tertiary nitrogen at the R2 chain. Irrespective of mode of administration, it blocks the osteoclast activity by inhibition of the mevalonate pathway after binding to the mineral phase of bone. Studies using animal models have shown a decrease in bone turnover and an increase in bone mass and bone strength, and that intermittent dosing provides the same benefits as continuous dosing regimens71. The potential for increasing the interval between doses has been studied in number of human phase II and III studies in an effort to find the optimal dosing interval with maintained effect on fracture and bone mass. The reports subsequently include different designs with regard to frequency and dose.
Effect on bone turnover
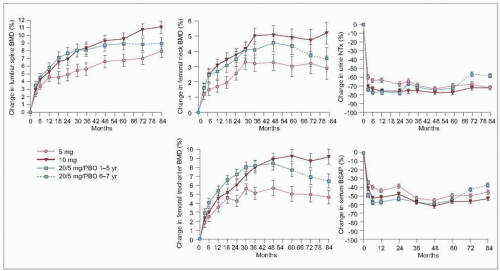
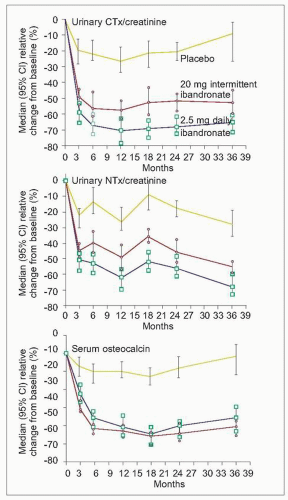
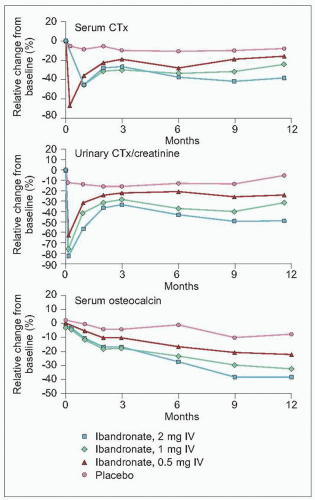
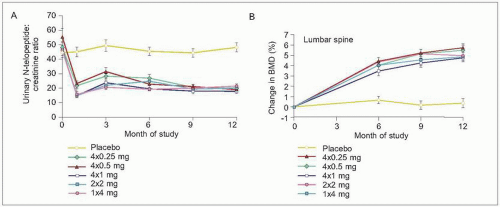
Bone markers serve as early indicator of effect in treatment studies of osteoporosis. In addition, they provide information on the pattern of metabolic response, which is even more interesting to describe when the dosing interval is increased. What occurs in the drug free interval? In a placebo-controlled study evaluating fracture efficacy and safety of daily oral and intermittent ibandronate, the effect on bone markers was also studied. The participants, postmenopausal women (n=2946, aged 55-80 years) were allocated into three groups: 2.5 mg ibandronate daily, 20 mg every other day for 12 days every third month, or placebo72. Blood samples were taken prior to dosing in those receiving intermittent dosing and therefore represents the residual effect. Bone resorption is markedly decreased during the entire 3 year treatment period73 (4.28). Both treatments led to a constant suppression of bone resorption, approximately 10% greater in those on daily compared to intermittent dosing. The response is less distinct when evaluated by urinary NTx for all treatments, suggesting a greater assay variability and not necessarily a drug effect, since the pattern is also similar for placebo. Bone formation is suppressed by about 40% but the plateau is delayed until 6 months.
For both bone resorption and bone formation markers, the response pattern is similar to that observed for other nitrogen-containing bisphosphonates. The response to intravenous intermittent dosing measured by bone markers shows a similar pattern. The suppression is dose-related and greater in those receiving 1 mg and 2 mg (4.29)74. Percentage-wise the suppression is somewhat less when ibandronate is administered intravenously, a finding possibly related to the fact that sampling is done just prior to the next dose and thus after 2-3 months without drug. However, with the 2 mg iv dose, bone resorption is decreased to 60% of baseline, a degree of suppression that is commonly aimed for when using oral bisphosphonates75. With monthly dosing, the suppression of bone turnover is significant and the higher concurrent dose (100 mg or 150 mg) induced a consistent >60% suppression76.
Effect on BMD
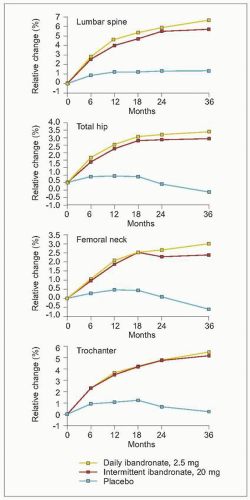
Oral daily and intermittent ibandronate produce significant increases in BMD at the spine and the hip as is shown in a 3-year RCT (4.30)72. Spinal BMD increase by 6.5% and 5.7%, respectively for 2.5 mg given daily and 20 mg given intermittently (see above), an increase that is of similar magnitude to that of other bisphosphonates. The increase is less pronounced in the hip (3.4% and 2.9%, respectively).
4.28 Ibandronate effect on bone markers. (Adapted from Delmas PD, et al. (2004). Daily and intermittent oral ibandronate normalize bone turnover and provide significant reduction in vertebral fracture risk: results from the BONE study. Osteoporos Int, 15(10):792-798.)
In the study by Chesnut et al.72, the intermittent dosing followed a regimen of 20 mg given for 12 consecutive days every 3 months, a dosing regimen that is suboptimal from a patient’s perspective despite a drug-free interval extending over 2 months. Modified dosing regimens have subsequently been developed and tested.
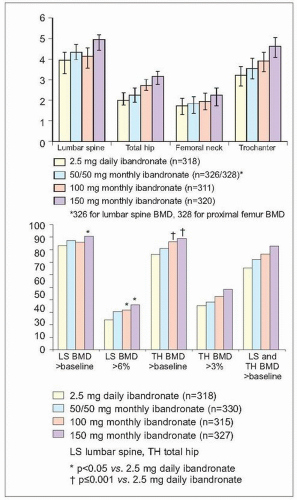
In a study of 1609 postmenopausal women, oral ibandronate was used: 2.5 mg daily, 50/50 mg (single dose on two consecutive days), 100 mg or 150 mg once monthly. The primary end-point was a BMD not significantly worse than baseline after 1 year of treatment76. Lumbar spine BMD increased by 4.1-4.9 % with the monthly regimens, and significantly more patients responded in the 150 mg group. The percentage change in hip BMD was similar, with a larger proportion in the 100 and 150 mg groups achieving a substantial increase (4.31, top). This study indicates that once-monthly oral ibandronate increases BMD over 1 year and is in this respect as effective as daily dosing. The proportion of patients responding is high, up to 90%, with the highest dose slightly superior (4.31, bottom).
4.29 Ibandronate effect on bone markers. (Adapted from Stakkestad JA, et al. (2003). Intravenous ibandronate injections given every three months: a new treatment option to prevent bone loss in postmenopausal women. Ann Rheum Dis, 62(10):969-975.)
4.30 Ibanronate effect on BMD. (Adapted from Chesnut III CH, et al. (2004). Effects of oral ibandronate administered daily or intermittently on fracture risk in postmenopausal osteoporosis. J Bone Miner Res, 19(8):1241-1249.)
4.31 Ibandronate effect on BMD. (Adapted from Miller PD, et al. (2005). Monthly oral ibandronate therapy in postmenopausal osteoporosis: 1-year results from the MOBILE study. J Bone Miner Res, 20(8):1315-1322.)
Effect on fracture
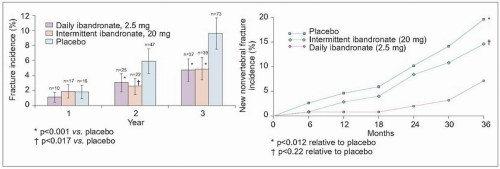
The only study to date sufficiently powered to evaluate the effect of ibandronate on fracture is the study by Chesnut et al.72, which included over 2900 women followed over 3 years, taking oral 2.5mg daily or 20 mg intermittent doses during a 3 monthly cycle. The relative risk reduction for incident radiographically identified vertebral fractures was 62% (95% CI 41-75) and 50% (95% CI 26-66) respectively, and both reached significance (p=0.0001, p=0.0006). There was no difference between continuous daily and intermittent dosing. The effect was significant during the second and third year of treatment (4.32, left). Close to 60% of the vertebral fractures presented as clinical fractures and the risk reduction for these women was 48-49% but statistically less secure (p<0.05). Nonvertebral fracture risk reduction was not associated with ibandronate treatment. Nevertheless, in a subgroup analysis, nonvertebral fracture risk in those with femoral neck BMD below T-score -3, fracture risk was lower by 69% (p<0.05) (4.32, right).
4.32 Ibandronate effect on fracture. (Adapted from Chesnut III CH, et al. (2004). Effects of oral ibandronate administered daily or intermittently on fracture risk in postmenopausal osteoporosis. J Bone Miner Res,19(8):1241-1249.)
Side-effects
Ibandronate will have a place in the therapy of osteoporosis, not from daily but from intermittent dosing and the benefits that are associated with dosing intervals of one or several months. From the perspective of convenience, it will not only be beneficial for the postmenopausal woman with an active lifestyle, but also for the very elderly where the disadvantage from complex dosing is even more evident. In this respect, side-effects are also of importance. These include gastrointestinal problems (30%), most commonly dyspepsia, musculoskeletal (27%), or general (25%)77. However, the side-effects and safety profile are comparable between all different dosing regimens and are no more common than in the placebo group. Intravenous administration may cause transient acute phase reaction, and a higher incidence of arthralgia and myalgia is reported78.
Zoledronate
The development of more potent bisphosphonates has also prompted the evaluation of their use in treating osteoporosis. Oral bisphosphonates have issues of compliance as well as problems of gastrointestinal tolerance, both of which have implications for their efficacy. Potent bisphosphonates which can be administered parenterally may avoid these issues.
Bisphosphonates are administered intravenously in patients with malignant hypercalcaemia and in those with Paget’s disease. Intermittent intravenous administration reduces skeletal events in breast cancer patients, with zoledronate associated with the largest risk reduction (RR 0.59, 95% CI 0.42-0.82)79. Zoledronic acid is the most potent bisphosphonate, 100-850-fold more potent than pamidronate. Like other nitrogen-containing bisphosphonates, it binds to the mineral phase of bone where it is internalized by osteosteoclasts, inhibiting farnesyl disphosphate synthase in the mevalonate pathway. The exact molecular mechanism of action is not clear; however, acidification is an absolute prerequisite80. Zoledronate is administered as an infusion over 15 minutes.
The majority of studies on zoledronate have been performed in patients with malignant conditions; however, intravenous bisphosphonates have also been used to alleviate pain in patients with Paget’s disease and to inhibit progression of the associated bone pathology. In a study comparing intravenous zoledronate with oral risedronate, the 6 month response rate was 96% in those receiving zoledronate and 74% in those receiving oral risedronate, as evaluated by change in alkaline phosphatase (p<0.001)81.
4.33 A Effect of zoledronate on bone markers. (Adapted from Reid IR, et al. (2002). Intravenous zoledronic acid in postmenopausal women with low bone mineral density. N Engl J Med, 346(9):653-661.) B Effect of zoledronate on BMD. (Adapted from Reid IR, et al. (2002). Intravenous zoledronic acid in postmenopausal women with low bone mineral density. N Engl J Med, 346(9):653-661.)
4.34 Effect of Zoledronate on fracture. (A Adapted from Black DM, et al. (2007). Onceyearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med, 356(18):1809-1822. B Adapted from Lyles KW, et al. (2007). Zoledronic acid and clinical fracture and mortality after hip fracture. N Engl J Med, 357(18):1799-1809.)
Effect on bone turnover
A first study on the use of zoledronate in postmenopausal osteoporosis included 351 women, assigned to four different dosing regimens or placebo and lasting for 12 months, used change in BMD as a primary end-point and bone markers as a secondary end-point82. The effect on bone turnover markers follows a pattern comparable to that of other potent bisphosphonates; most pronounced for resorption markers and to a lesser extent for formation markers, with resorption markers rapidly suppressed with a maximum decrease at 1 month; serum C-telopeptide decreased by a median of 65-83% and urine N-telopeptide by 50-69% (4.33A)82.
Effect on BMD
The protocol of the initial study included a single yearly dose of 4 mg or a divided dose of 2 mg, two times over a year. Four different dose regimens of zoledronate produced similar effects on bone density (4.3-5.1% at the lumbar spine) after 12 months. Notably, the single annual intravenous dose of 4 mg zoledronic acid gave the same increase as more frequent dosing 82 (4.33B). Clearly, it was possible to administer one yearly dose or biannual doses of a potent bisphosphonate and still achieve significant effects. This was later confirmed, where annual infusions of zoledronic acid lead to BMD increases of 5-7% over 3 years83.
Effect on fracture
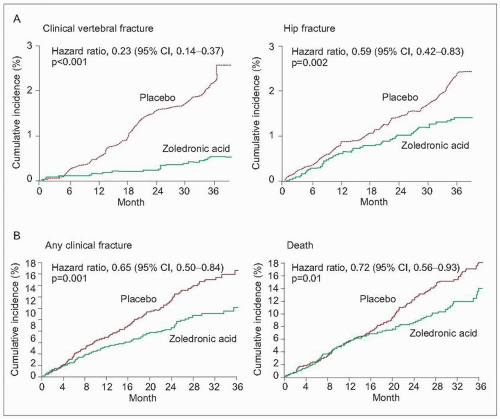
To evaluate the effect on fracture, a large-scale randomized controlled study has been performed in women with postmenopausal osteoporosis (n=3889)83. With a mean age of 73 years, this is a population at somewhat higher risk compared to similar studies of oral bisphosphonates. After 3 years of annual 5 mg zoledronic acid infusions, the relative risk of clinical vertebral fractures was reduced by 77% (p<0.001), and nonvertebral fractures, all clinical fractures, and hip fracture by 25%, 33% and 41% respectively (4.34A). In absolute terms 2.5% (n=88) in the placebo group and 1.4% (n=52) in the treated group suffered a hip fracture.
Hip fracture patients have a high risk of recurrent fractures; in a randomized, double-blinded, placebo controlled study including 1065 hip fracture patients, zoledronic acid was given 90 days after fracture84. A 35% reduction of any clinical fracture was evident (p=0.001), as was a 46% decrease in clinical vertebral fractures (p=0.02) (4.34B). Furthermore, mortality was reduced by 28% among those treated with zoledronic acid (p=0.01).
Side-effects
Among side-effects, the major difference in all reported studies, is the experience of influenza-like symptoms, e.g. acute phase reaction within the first 3 days after intravenous administration – in postmenopausal women 32-54% and in hip fracture patients 7%. Common complaints included musculoskeletal pain, fever, and nausea and most occurred during the first time administration of the drug, while to a much lesser extent at subsequent infusions. A nonexplained increase in atrial fibrillations was seen in postmenopausal women, but not in hip fracture patients83, 84.
In summary, current data on zoledronate for the treatment of osteoporosis support a beneficial effect on BMD and a significant reduction in both vertebral and nonvertebral fractures.
Tiludronate is a third generation, non-nitrogen containing bisphosphonate that can be administered either orally or intravenously and has mainly been used in the treatment of Paget’s disease; after initially promising results, it has not been further developed for use in osteoporosis.
Hormone replacement therapy
Oestrogen is important both for skeletal development and structural maintenance of bone. The balance between bone resorption and bone formation in adulthood is in part dependent on intact oestrogen levels, and bone loss during the initial years after menopause is linked to oestrogen withdrawal. Oestrogen exhibits its effect on both osteoblasts and osteoclasts through several mechanisms, but action via the oestrogen receptors (ER) is probably most important. Two ERs are identified, and ERα.alpha; appears to be the main receptor associated with bone.
The rapidly decreasing oestrogen levels at menopause may lead to increased activation frequency, that is the number of active resorption sites increase while the capacity to refill the site with new bone diminishes, causing bone loss. By substituting for oestrogen loss or manipulating the ER activity, the rate of bone turnover should remain in balance. This is the rationale for the use of oestrogen replacement therapy (ERT) and for the development of new drugs that modify the ER.
Oestrogen replacement
Oestrogen replacement therapy (ERT) has been widely used for many years to alleviate postmenopausal symptoms related to oestrogen withdrawal, with the additional effect on bone turnover and bone mass. The effect on fracture by ERT has been evaluated in meta-analysis of randomized trials finding a reduction in nonvertebral fractures of 27%85 and in vertebral fractures of 33%86. The effect was less clear in older women. There is an offset of benefit; thus the advantages of taking hormone replacement therapy (HRT) while the woman is in her 50s on fracture risk at the peak age of 70-80 years is unclear. The recent Women’s Health Initiative (WHI) study, which recruited 16,608 healthy postmenopausal women aged 50-79 years, found that ERT reduced the risk of both vertebral and hip fracture. The bone density was unknown at the start of the study.
Table 4.6 Summary of risks and benefits associated with using HRT
Condition
Age of woman (years)
Number of cases/1000 nonHRT users
Extra number of cases in 1000 HRT users for 5 years HRT use over the same period*
Reduced number of cases in 1000 HRT users over the same period
Colorectal
50-59
6
3
No significant effect
1 (±1)
cancer
60-69
10
8
3 (±2)
Fracture of neck
50-59
0.5
1.5
0.3 (±0.51)
0.3 (±1)
of femur
60-69
5.5
5.5
3 (±2)
3 (±2)
Numbers are best estimates (± approximate range from 95% CI)
* All values are from the WHI trial unless otherwise stated
a CA cumulative risk of 14 cases/1000 non-HRT users over 5 years has been used to facilitate comparison of the MWS and the WHI studies
b Estimates from the placebo group of the WHI trial
c Relative risk associated with 5 years’ use of oestrogen-only HRT (RR = 2.8 (2.3-3.5) from metaanalysis)
d Risk cannot be reliably estimated – the addition of a progestogen for at least 12 days per month greatly reduces the additional risk of endometrial cancer due to unopposed oestrogen, but the magnitude of the reduction is poorly defined at present
The major concern for the role of ERT in the prevention of osteoporosis and fracture is the increased risk of breast cancer, endometrial cancer, ovarian cancer, stroke, and venous thromboembolism (Table 4.6). The risks and benefits and individual circumstances, therefore, have to be carefully considered when recommending ERT, and the duration of treatment should stay within 5 years for a postmenopausal woman in most circumstances.
It is common practice to use ERT in premature oestrogen deficiency to ensure adequate levels up to the expected age of menopause as these women may otherwise be at increased risk of future fracture. However, there is little evidence for the long-term benefits of this approach. Oestrogen should be given opposed with either cyclic or continuous gestagen to women with an intact uterus, as there is otherwise an increased risk of endometrial cancer.
Selective oestrogen receptor modulators
Oestrogen plays an important role in the maintenance of skeletal integrity in women and probably also in men. Oestrogen exhibits agonistic effects, whereas selective oestrogen receptor modulators (SERMs) have both agonistic and antagonistic effects in tissues responsive to oestrogen. SERMs are nonsteroidal ligands that produce agonistic effects in bone, similar to those of oestrogen, but antagonistic effects in, for example, breast tissue. Raloxifene has been evaluated in major trials for treatment of osteoporosis and breast cancer, alongside substudies evaluating the effects on other organ systems.
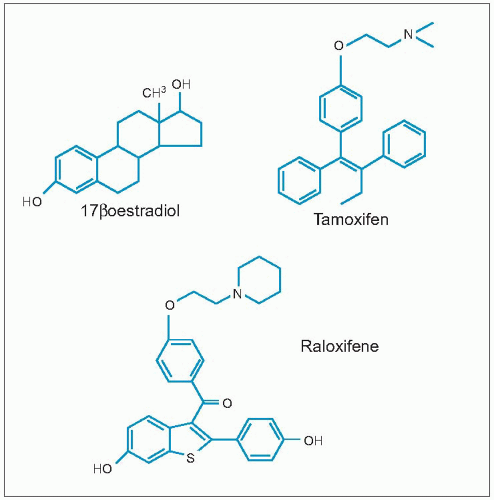
In addition to the significant antioestrogenic effect on breast tissue from tamoxifen, a pronounced effect was also recognized in uterine tissue, as was a weak agonistic effect on bone. When raloxifene was developed it was discovered that it provided not only a minimal uterine response, but also a significant inhibition of bone resorption87. Both tamoxifen and raloxifene bind to the oestrogen receptor, despite different primary structures compared to oestrogen (4.35)88.
Mechanisms of action
Oestrogen binds to the oestrogen receptor, inducing conformational changes of the receptor and forming an oestrogen receptor-oestrogen complex that diffuses into the nucleus89. Raloxifene acts as a competitive ligand to oestrogen receptor, blocking the conformational changes of the receptor modulating the gene activation and subsequent protein production. Raloxifene can bind to both oestrogen receptor-α and oestrogen receptor-β, but has a four-fold greater affinity for oestrogen receptor-α90.
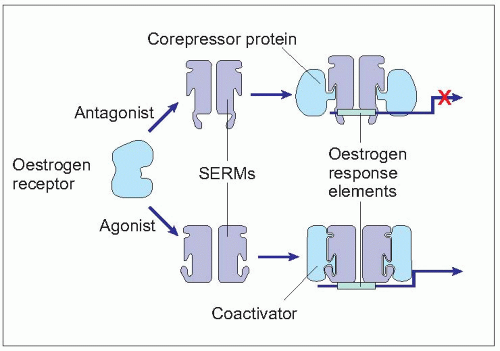
When oestrogen receptor-SERM binds in tissues where a primarily agonistic expression is expected (such as bone for raloxifene), the receptor-ligand complex acts preferentially via a coactiviator enhancing the agonistic effect (4.36). When oestrogen receptor-SERM binds in tissues where a primarily antagonistic expression is expected (such as breast for raloxifene), the receptor-ligand complex acts preferentially via a corepressor enhancing the antagonistic effect91.
Effect on bone turnover
Raloxifene reduces urinary calcium excretion, conferring a positive calcium balance92 and decreases bone turnover as assessed by bone markers93. The decrease in bone markers of between 30-40% indicates that raloxifene is primarily an antiresorptive agent; however, this is a less pronounced decrease compared to what is seen with bisphosphonates94, 95.
4.35 Structure of oestrogen in relation to raloxifene.
4.36 SERM and mechanisms of action.
Raloxifene inhibits bone resorption as indicated in animal studies; however, the exact mechanism remains to be elucidated. The effect on bone turnover is that of an antiresorptive agent with levels of bone markers decreasing during the first 6-9 months. The change in bone markers over 24 months of raloxifene at three different doses vs. placebo is clear93. The mean decrease after 24 months of raloxifene treatment was 15-23% for bone formation and 34% for bone resorption in those receiving the 60 mg dose.
Only gold members can continue reading. Log In or Register to continue