 Lateral Approach to the Hind Part of the Foot
Lateral Approach to the Hind Part of the FootThe lateral approach provides excellent exposure of the talocalcaneonavicular, posterior talocalcaneal, and calcaneocuboid joints. It permits arthrodesis of any or all these joints (triple arthrodesis).
Position of the Patient
Position the patient supine on the operating table. Place a large sandbag beneath the affected buttock to rotate the leg internally, and bring the lateral portion of the ankle and hind part of the foot forward. Further increase internal rotation by tilting the table away from you. Exsanguinate the limb either by elevating it for 5 minutes or by applying a soft rubber bandage, and then inflate a tourniquet (see Fig. 7-1).
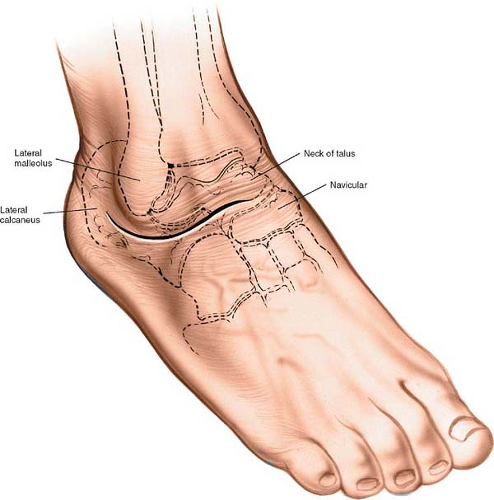 Figure 10-1 Make a curved incision starting just distal to the distal end of the lateral malleolus and slightly posterior to it. Continue distally along the lateral side of the hind part of the foot and over the sinus tarsi. Then, curve the incision medially toward the talocalcaneonavicular joint. |
Landmarks and Incision
Landmarks
The lateral malleolus is the palpable distal end of the fibula. The lateral wall of the calcaneus is subcutaneous. It is palpable below the lateral malleolus.
To palpate the sinus tarsi, stabilize the foot, holding the calcaneus with one hand, and place the thumb of the free hand in the soft-tissue depression just anterior to the lateral malleolus. The depression lies directly over the sinus tarsi.
Incision
Make a curved incision starting just distal to the distal end of the lateral malleolus and slightly posterior to it. Continue distally along the lateral side of the hind part of the foot and over the sinus tarsi. Then, curve medially, ending over the talocalcaneonavicular joint (Fig. 10-1).
Internervous Plane
The internervous plane lies between the peroneus tertius tendon (which is supplied by the deep peroneal nerve) and the peroneal tendons (which are supplied by the superficial peroneal nerve).
Superficial Surgical Dissection
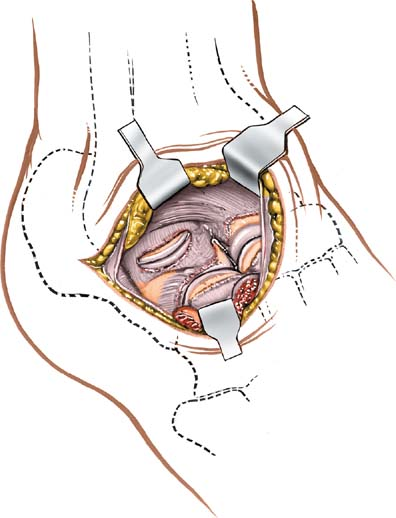
Do not mobilize the skin flaps widely, because large skin flaps may necrose. Ligate any veins that cross the operative field. Open the deep fascia in line with the skin incision, taking care not to damage the tendons of the peroneus tertius and extensor digitorum longus muscles, which cross the distal end of the incision (Figs. 10-2 and 10-3). Retract these tendons medially to gain access to the dorsum of the foot. Do not retract the peroneal tendons, which run through the proximal end of the wound, at this stage (Fig. 10-4).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


