The median nerve provides sensory innervation to the radial aspect of the hand, including the palm, thumb, index, long, and half of the ring fingers. It provides motor innervation to most of the volar forearm musculature and, importantly, to m ost of thenar musculature. The main goal of median nerve reconstructive procedures is to restore thumb opposition. There are a variety of transfers that can achieve this goal but tendon transfers must recreate thumb opposition, which involves 3 basics movements: thumb abduction, flexion, and pronation. Many tendon transfers exist and the choice of tendon transfer should be tailored to the patient’s needs.
- •
Median nerve injuries are classified as low and high and many more options exist for low median nerve palsies.
- •
Restoration of thumb opposition is the main goal of reconstructive surgery.
- •
Successful tendon transfers recreate thumb opposition, which involves 3 basic movements: thumb abduction, flexion, and pronation.
- •
Loss of sensation to the median aspect of the hand is a relative contraindication to tendon transfer.
Introduction
Median nerve palsy is arguably one of the most debilitating injuries to the hand, particularly if the ability to achieve thumb opposition is lost. Most reconstructive operations for late median nerve palsies are aimed at restoration of motor function and thumb opposition. Outcomes of any late reconstruction are often dictated by the amount of sensation that has been restored. Median nerve palsies are classified as “high” or “low” based on their anatomic location. Many reconstructive options exist but are limited by the location of the lesion and other associated injuries.
Anatomy
The median nerve arises from the medial and lateral cords of the brachial plexus. It does not give off any motor or sensory branches until it courses distal to the cubital fossa. At this point, the nerve pierces and innervates the 2 heads of the pronator teres muscle. In the forearm, the median nerve travels between flexor digitorum superficialis (FDS) and the flexor digitorum profundus (FDP) muscle bellies. Motor branches extend to FDS, flexor carpi radialis, and palmaris longus. A major motor branch, the anterior interosseous nerve (AIN), separates to innervate flexor pollicis longus (FPL), pronator quadratus, and FDP to the index and long fingers. The palmar cutaneous nerve branches off in the forearm approximately 5 cm proximal to the wrist flexion crease, providing sensation to the radial aspect of the palm. The remaining nerve travels through the carpal tunnel, where the recurrent motor branch innervates the intrinsic thenar muscles, including abductor pollicis brevis (APB), opponens pollicis, and the superficial head of flexor pollicis brevis (FPB). The deep head of the FPB is innervated by the ulnar nerve. Additional median motor branches innervate the lumbricals of the index and middle fingers. Sensory branches exiting distal to the carpal tunnel provide sensation to volar aspect of the thumb, index, middle, and radial half of the ring fingers.
Anatomy
The median nerve arises from the medial and lateral cords of the brachial plexus. It does not give off any motor or sensory branches until it courses distal to the cubital fossa. At this point, the nerve pierces and innervates the 2 heads of the pronator teres muscle. In the forearm, the median nerve travels between flexor digitorum superficialis (FDS) and the flexor digitorum profundus (FDP) muscle bellies. Motor branches extend to FDS, flexor carpi radialis, and palmaris longus. A major motor branch, the anterior interosseous nerve (AIN), separates to innervate flexor pollicis longus (FPL), pronator quadratus, and FDP to the index and long fingers. The palmar cutaneous nerve branches off in the forearm approximately 5 cm proximal to the wrist flexion crease, providing sensation to the radial aspect of the palm. The remaining nerve travels through the carpal tunnel, where the recurrent motor branch innervates the intrinsic thenar muscles, including abductor pollicis brevis (APB), opponens pollicis, and the superficial head of flexor pollicis brevis (FPB). The deep head of the FPB is innervated by the ulnar nerve. Additional median motor branches innervate the lumbricals of the index and middle fingers. Sensory branches exiting distal to the carpal tunnel provide sensation to volar aspect of the thumb, index, middle, and radial half of the ring fingers.
Classification
The classification of median nerve palsies is based on the anatomic location of the lesion.
Low median nerve palsies are typically described as lesions that occur distal to the origin of the AIN. Functionally, this affects the thenar musculature and median innervated intrinsic, resulting in loss of thumb opposition and sensory loss in the median nerve distribution as described earlier. In part, because the FPB has duel innervation from both the median and the ulnar nerve, not all patients with isolated median nerve palsy will experience complete loss of thumb opposition.
High median nerve palsies are lesions that occur proximal to the origin of the AIN. In addition to potentially creating the same motor and sensory deficits as low median nerve injuries, high median nerve lesions affect the muscles of the forearm. Functionally, this results in diminished forearm pronation from denervation of the pronator teres and pronator quadratus and loss of thumb interphalangeal (IP) joint flexion from denervation of FPL. Patients can also experience wrist flexion weakness from denervation of the flexor carpi radialis and grip strength as a result of the denervation of FDS and FDP to the index and middle fingers. High median nerve lesions are more functionally debilitating and difficult to recover from. They also have implications for the potential reconstructive options for median nerve palsies given their greater functional deficits.
Causes
There are many causes of median nerve palsies, and they can broadly be characterized into traumatic, compressive, congenital, and other diseases affecting sensory and motor function. Traumatic causes include direct nerve laceration or contusion and brachial plexus injuries. Compressive causes most commonly include carpal tunnel and radiculopathy from nerve root compression. Although it is not technically considered a palsy, congenital absence of the thenar muscles can result in similar functional deficits as median nerve lesions and require similar reconstructive operations. Many other diseases can affect median nerve function, including Charcot-Marie-Tooth, leprosy, syringomyelia, spinal muscular atrophy, Guillain-Barre, and polio. Although it is currently more of historical interest, polio was once considered to be the most ideal indication for reconstructive opponensplasty for median nerve palsy because it is purely a motor deficit.
Indication for surgery
Most reconstructive options that are currently used for late median nerve palsy are aimed at the restoration of thumb opposition. As noted, because of variations in anatomy and the patient’s ability to compensate, functional loss of opposition is not present in all median nerve palsies, even when the nerve is completely transected. Jensen reported that opponensplasty was needed in only 14% of the patients he encountered. Additionally, loss of thumb opposition may not present a large functional barrier for some patients, particularly if they have low functional demands or the deficit involves the nondominant hand.
If a nerve deficit results from a direct laceration, direct repair or grafting should be the first line of treatment. This may allow for sufficient functional recovery such that reconstruction is not needed and provides the best chance for sensation to be restored. In cases whereby direct repair is not possible or functional loss of opposition remains despite repair, reconstructive surgery may be indicated. It should be noted that permanent sensory loss might compromise the functional outcome of any reconstructive operation even if it is technically successful. Therefore, some surgeons consider loss of thumb sensibility to be a relative contraindication to reconstructive surgery. However, others have advocated for early surgery despite sensory loss, noting that tendon transfers serve as internal splints and eyesight compensates for sensory loss.
In addition to these considerations, the general principles of tendon transfer must be respected. The importance of these basic principles of tendon transfer cannot be overstated and will ensure optimal clinical outcomes. They are listed here:
- 1.
A tendon transfer should not be performed in the presence of an unhealed wound.
- 2.
The full passive joint motion must be restored before tendon transfer.
- 3.
Transfer should not pass through areas of scar tissue or under skin grafts, and surgical incisions should not be placed directly over the transfer.
- 4.
Cutaneous sensation should be restored before the tendon transfer, if possible.
- 5.
The normal function of the transferred muscle must be expendable.
- 6.
The transferred muscle must be under voluntary control and have an independent action.
- 7.
The transferred muscle must have sufficient amplitude and power to perform its new function; thus, reinnervated muscles should be used only in exceptional circumstances.
- 8.
If the transfer cannot perform its new function with a straight line of pull from its origin to its insertion, it should pass through no more than one pulley. Acute angulation of the transfer at the pulley should be avoided.
- 9.
Synergism between the muscle’s original and new actions facilitates rehabilitation.
Principles of opponensplasty
The mechanics of thumb opposition involves 3 basic movements: thumb abduction, flexion, and pronation. The APB primarily drives opposition, although there is some modest contribution from the opponens pollicis and FPB. In 1938, Bunnell published the essential principles of opponensplasty that complement the general principles of tendon transfer. First, he noted that the direction of pull of a transferred tendon should be from the direction of the pisiform bone. Second, he stated that the insertion of the tendon transfer should be on the dorsoulnar aspect of the proximal phalanx of the thumb so that the transfer can more accurately restore thumb pronation. These principles are still generally adhered to today although the distal insertion site now used for most tendon transfers is at the dorsoradial aspect of the proximal phalanx near the anatomic insertion of the APB tendon and thumb extensor expansion. More recent studies have demonstrated that adequate thumb pronation is still achieved with this insertion site.
Specific opponensplasties for late median nerve palsies
Bunnell Opponensplasty (Ring Finger FDS Transfer)
The ring finger FDS tendon transfer was originally conceived by Royle in 1938. In his original description, the ring FDS tendon was detached from its insertion site on the middle phalanx, retrieved via a secondary incision at the wrist flexion crease, and rerouted through the FPL tendon sheath. Thompson later modified this technique in 1942 so that the ring FDS tendon was rerouted subcutaneously to the thumb base instead of through the FPL tendon sheath. It was later appreciated that detaching the FDS tendon from its insertion site made the proximal IP joint prone to contractures and swan neck deformities. The current recommendation is that the tendon be harvested between the A1 and A2 pulley near the metacarpophalangeal (MP) joint.
Bunnell was the first to describe the technique most commonly used today in which a slip of the flexor carpi ulnaris (FCU) tendon is used to create a fixed pulley for the ring FDS tendon to pass through. This creates a direction of pull near the pisiform as previously noted. Other pulley sites have also been proposed, including the angle at the distal edge of the flexor retinaculum, Guyon canal, and the ulnar border of the palmar aponeurosis. Multiple possible pulley site options allow the surgeon to customize a transfer to address a patient’s specific functional deficit. Pulley sites near the pisiform produce the most thumb abduction and opposition, whereas pulley sites distal to this increase the amount of thumb MP joint flexion that can be achieved.
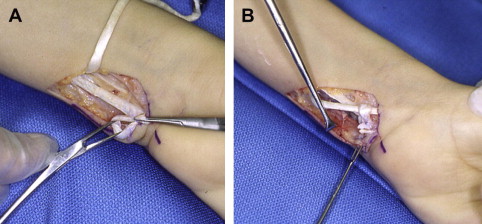
The surgical technique involves first releasing the ring FDS tendon distally, most commonly between the A1 and A2 pulley. A secondary incision is then made just proximal to the wrist crease over the FCU tendon. A distally based radial slip of the FCU tendon is created, leaving about 4 cm of tendon attached to its insertion on the pisiform. A distally based slip has been shown to best prevent pulley migration. The proximal end of the slip is used to create a loop (pulley) and is sewn to itself at the distal insertion on the pisiform ( Fig. 1 ). A third incision is made over the dorsal aspect of the thumb MP joint. A subcutaneous tunnel is developed from the loop to the thumb incision to allow passage of the ring FDS. The tendon is passed through the tunnel and inserted into a bone tunnel on the dorsoulnar aspect of the base of proximal phalanx. This is Bunnell’s original description, although other insertion sites, such as suturing to the APB tendon insertion without making a bone tunnel, can also be used. Tensioning of the tendon transfer is critical and must be set such that the thumb is fully opposed when the wrist is in a neutral position.
Related posts:
 Electrodiagnostic Evaluation of Compressive Nerve Injuries of the Upper Extremities
Late Reconstruction of Ulnar Nerve Palsy
Ulnar Tunnel Syndrome
Physical Examination of Upper Extremity Compressive Neuropathies
Open Versus Endoscopic Carpal Tunnel Release
Ulnar Neuropathy Following Distal Humerus Fracture Fixation
Electrodiagnostic Evaluation of Compressive Nerve Injuries of the Upper Extremities
Late Reconstruction of Ulnar Nerve Palsy
Ulnar Tunnel Syndrome
Physical Examination of Upper Extremity Compressive Neuropathies
Open Versus Endoscopic Carpal Tunnel Release
Ulnar Neuropathy Following Distal Humerus Fracture Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


