Lateral trunk flexion (LTF) often occurs in Parkinson disease (PD). Recently, 2 possible mechanisms for the pathogenesis of Pisa syndrome have been proposed: a segmental deficit of motor tone resulting from imbalanced basal ganglia functioning or a deficit in spatial cognition including correct body orientation in relation to gravity and the integration of information from visual, vestibular and somaesthetic sources . Most postural abnormalities are managed by modifying dopaminergic medication or physiotherapy. Deep brain stimulation or botulinum toxin injection was often effective, but managing postural deviations remains a challenge .
Electromyography and radiology investigations have shown 2 different patterns of unilateral hyperactivity and unilateral hypertrophy in PD patients with LTF: ipsilateral or contralateral to the LTF side . Similarly, camptocormia is associated with different patterns of the gradient of trunk flexion during walking , and surface electromyography has revealed the involvement of the external oblique and psoas major muscles in the development of upper and lower camptocormia . In patients with LTF, such findings are limited to muscles such as the obliquus abdominis or thoracic paraspinal muscles or several other extra-abdominal muscles.
Recently, we reported that in PD patients with LTF, the lumbar quadrate or psoas major muscle of the intra-abdominal muscles showed 2 hypertrophic patterns, contralateral or ipsilateral to the leaning side, and proposed that the hypertrophic muscle ipsilateral to the bending side might be a new therapeutic target . Here, we describe a case of PD with left-sided LTF subsequently presenting right-sided LTF, accompanied by an increase in muscle size of the left-sided lumbar quadrate muscle.
In April 2013, a 62-year-old right-handed man noticed a tremor in his left hand. In November 2014, he presented left-sided LTF and difficulty walking. The diagnosis was PD. Treatment with levodopa was started, and the dose was increased to 450 mg/day, but LTF developed. The uptake ratio of 123 I-metaiodobenzylguanidine in the heart-mediastinum was significantly decreased. Cranial MRI findings were normal. In February 2015, treatment with rotigotine (4.5 mg/day) was started.
In April, the LTF was unchanged, and the patient consulted at our hospital. He showed signs and symptoms of mild PD, including masked face, akinesia, left-sided dominant rigidity in 4 limbs, and left-sided LTF ( Fig. 1 a) . The scores on parts III and IV of the unified PD rating scale (UPDRS) were 17 and 0, respectively. Mini-Mental State Examination results were normal. The dose of rotigotine was increased to 9 mg/day, and the severity of LTF and left-sided rigidity in upper and lower limbs was slightly decreased. In November, right-sided LTF developed over 2 weeks ( Fig. 1 b). The scores on parts III and IV of the newly revised UPDRS were 20 and 0, respectively, and right-sided dominant rigidity in 4 limbs was evident.
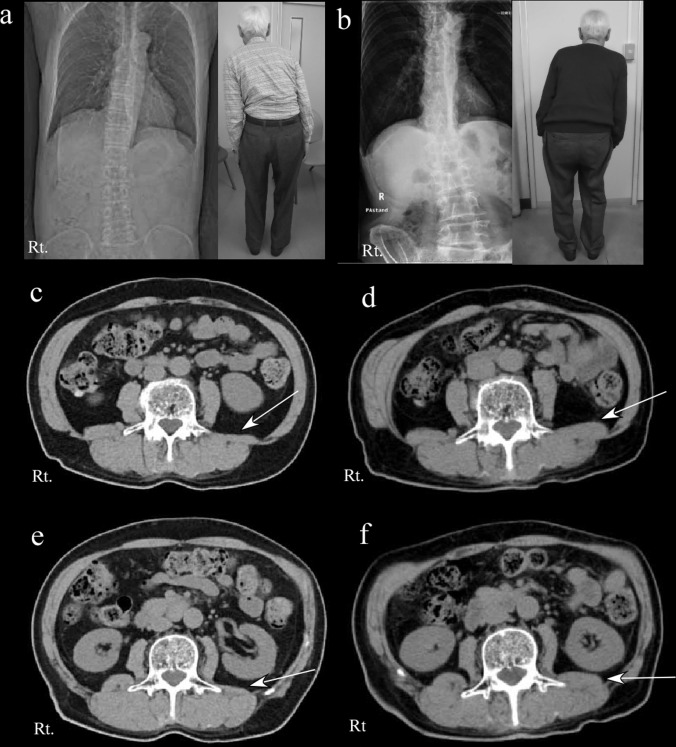
During the LTF, mild to moderate back and lumbar pain was evident. We performed axial plane CT scanning at the L3 and L4 vertebral levels with the patient in the supine position to determine whether paired muscles showed unilateral differences in muscle areas. The first CT scan was obtained 5 months after the onset of left-sided LTF ( Fig. 1 c and e) and the second CT scan at 3 weeks after the onset of right-sided LTF ( Fig. 1 d and f). By using the axial CT images obtained at the middle margin of the L4 and L3 vertebral levels, we analyzed regions of interest in the right and left lumbar quadrate muscle, psoas major muscles, paravertebral muscles, and internal and external abdominal oblique muscles ( Table 1 ). The change in muscle areas between the first CT scan (at the time of left-sided LTF) and the second CT scan (at the time of right-sided LTF) was particularly remarkable for the left lumbar quadrate muscles (from 269.78 to 571.08 mm 2 at the L4 level and from 208.34 to 404.10 mm 2 at the L3 level). This change in muscle area was slight in the psoas major muscle, paravertebral muscles, and internal and external abdominal oblique muscles. These investigations were reliable because 2 different CT scans performed with same slice thickness showed similar horizontality, and the analysis of region of interest was calculated repeatedly.
| Muscle area | Right side | Left side | Difference (mm 2 ) ( B − A ) b | ||||
|---|---|---|---|---|---|---|---|
| First CT (mm 2 ) | Second CT (mm 2 ) | Difference, (mm 2 ) ( A ) a | First CT (mm 2 ) | Second CT (mm 2 ) | Difference (mm 2 ) ( B ) a | ||
| L4 level | |||||||
| Lumbar quadrate muscle | 504.7 | 415.8 | −88.9 | 269.8 | 571.1 | 301.4 | 390.3 |
| Psoas major muscle | 772.2 | 616.5 | −155.7 | 756.6 | 634.3 | −122.3 | 33.5 |
| Internal abdominal oblique muscles | 959.5 | 868.5 | −90.9 | 879.3 | 757.8 | −121.5 | 30.7 |
| External abdominal oblique muscles | 1055.3 | 902.0 | −153.3 | 653.9 | 568.8 | −85.2 | 68.1 |
| Paravertebral muscles | 2478.2 | 2041.2 | −437.0 | 2261.9 | 1877.5 | −384.4 | 62.6 |
| L3 level | |||||||
| Lumbar quadrate muscle | 413.9 | 367.7 | −46.1 | 208.3 | 404.1 | 195.8 | 241.9 |
| Psoas major muscle | 568.5 | 443.2 | −125.2 | 530.8 | 481.5 | −49.2 | 76.0 |
| Internal abdominal oblique muscles | 789.9 | 696.8 | −93.1 | 674.4 | 613.7 | −60.7 | 32.4 |
| External abdominal oblique muscles | 1074.0 | 790.9 | −283.1 | 845.7 | 641.9 | −203.8 | 79.3 |
| Paravertebral muscles | 2473.8 | 2218.3 | −255.4 | 2238.3 | 1990.7 | −247.7 | 7.8 |
| LTF side | Left | Right | Left | Right | |||
Related posts:
 Complex regional pain syndrome associated with hyperattention rather than neglect for the healthy side: A comprehensive case study
Complex regional pain syndrome associated with hyperattention rather than neglect for the healthy side: A comprehensive case study
 Validation of a novel activity monitor in impaired, slow-walking, crutch-supported patients
Care-related pain and discomfort in children with motor disabilities in rehabilitation centres
Validation of a novel activity monitor in impaired, slow-walking, crutch-supported patients
Care-related pain and discomfort in children with motor disabilities in rehabilitation centres
 Restoration of normal swallowing function in Wallenberg syndrome by repetitive transcranial magnetic stimulation and surgery
An update on the pathophysiology of osteoarthritis
Does the physiatrist replicate the functions of the neurologist or orthopedist?
Restoration of normal swallowing function in Wallenberg syndrome by repetitive transcranial magnetic stimulation and surgery
An update on the pathophysiology of osteoarthritis
Does the physiatrist replicate the functions of the neurologist or orthopedist?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


