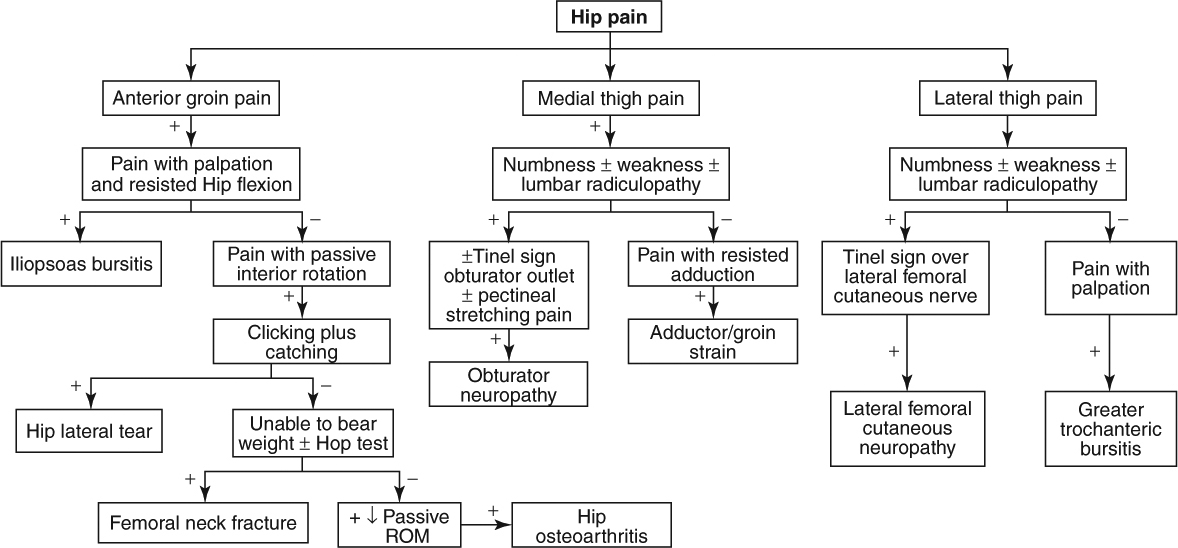
Hip and Groin Pain
|
Red Flag Signs and Symptoms
Any of these signs and symptoms should prompt urgent evaluation and appropriate intervention:
Fevers
Chills
Hot, swollen joint
Progressive neurologic symptoms
Loss of pulses
GROIN STRAIN
Background
The muscles of the inner thigh consist of the adductor magnus, adductor longus, and adductor brevis. This muscle group is commonly injured in sports that require lateral movement or pivoting. Sudden forced abduction of the hip usually causes injury to the inner thigh or groin. Usually minor tears occur in the muscle belly causing severe pain.
Clinical Presentation
Usually patients present with pain localized to the inner thigh. Depending on the severity of the injury, patients may complain of difficulty with sport-specific activity, normal walking, or at rest. Pain is exacerbated by lateral movement or pivoting.
Physical Examination
The patient’s pain is usually elicited with resisted adduction. The FABER (flexion abduction external rotation) (Patrick) test (Fig. 6.1) also reproduces the patient’s pain. In addition, palpation of the muscle may reproduce the patient’s pain. Examination of ambulation may reveal an antalgic gait.
 Figure 6.1 FABER (Patrick) test. |
Diagnostic Studies
Usually imaging studies are not needed to diagnose strain. If the pain persists after an adequate amount of rest, physical therapy, ice, and medication, magnetic resonance imaging (MRI) may be needed to assess the soft tissue.
Treatment
Rest, ice, compression, and elevation (RICE) is the initial treatment of any strain. Usually patients are instructed to rest for 4 to 6 weeks to allow moderate to severe
strains to heal. Medications such as anti-inflammatories are useful in treating pain and the inflammation that may be present. If the pain continues despite adequate rest, the use of a thigh sleeve to help contain the muscle is effective.
strains to heal. Medications such as anti-inflammatories are useful in treating pain and the inflammation that may be present. If the pain continues despite adequate rest, the use of a thigh sleeve to help contain the muscle is effective.
HIP OSTEOARTHRITIS
Background
As many as 25% of people may develop hip osteoarthritis (OA) at some point in their life according to the Johnston County Osteoarthritis Project. This risk is increased in people who are overweight or obese. Previous trauma to the hip also increases risk. As in other body parts, osteoarthritis is characterized by articular cartilage loss.
Clinical Presentation
Patients classically present with groin pain. The pain also may refer into the anterior thigh, buttock, or knee. Pain is initially aggravated by walking and climbing stairs. As the disease progresses, pain may be present at rest and nighttime. Patients may complain of limping because of the pain.
Physical Examination
An antalgic gait may be noted with the patient favoring the uninvolved side. The hallmark physical examination finding is loss of internal rotation as well as reproduction of symptoms with internal rotation and external rotation. Range of motion while loading the joint is also a good test. For this examination maneuver, the patient lies supine and the physician rotates the hip internally and externally while compressing the femur into the acetabulum with a downward pressure on the knee.
Diagnostic Studies
Radiographs should be obtained and may reveal asymmetric joint space narrowing, osteophytes, subchondral cyst, and/or sclerosis (Fig. 6.2). Importantly, radiographic findings do not necessarily correlate with severity of disease. Radiographs may reveal significant arthritis but the patient may have minimal symptoms. Reciprocally, radiographs may be normal and symptoms significant.
 Figure 6.2 Radiograph of hip osteoarthritis. (From Moskowitz et al. Osteoarthritis Diagnosis and Medical/Surgical Management. 4th ed. Philadelphia, Pa: Lippincott Williams & Wilkins, 2007, with permission.) |
MRI may be more sensitive and specific for osteoarthritis in terms of evaluating the cartilage. However, this costly test is not practical or needed in most cases of hip OA.
Treatment
Physical therapy is the cornerstone of treatment. When a hip becomes arthritic and painful, the patient’s inclination may be not to use it. However, disuse does not allow needed nourishment to get to the remaining cartilage, leading to further quickening cartilage loss. Physical therapy works on strengthening the supporting musculature of the hip, as well as improving core stabilization, and addresses any flexibility limitations.
The patient should be encouraged to listen to their body but try and stay active. Weightbearing exercises that are nonimpact are ideal. Using an elliptical machine is an excellent example. Alternatively, nonweightbearing exercises are also good. These would include swimming or riding the stationery bike. Impact exercises are all right to do and are certainly better than doing no exercises, but they may be too painful. Patients must listen to their body to help guide them in terms of which exercises to perform.
Nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen can also be helpful for mild pain relief. Oral supplementation with glucosamine and chondroitin sulfate and topical analgesic creams may also be helpful.
Intra-articular injections of corticosteroid and anesthetic can be very effective in reducing symptoms of hip OA. The injections should be done under fluoroscopic or ultrasound guidance. Ideally, the injection (as well as all analgesic medications) is used as a bridge to reduce the pain and allow the patient to participate more fully with physical therapy. Intra-articular hyaluronic acid injections also appear promising in treating hip OA, although more research is needed.
When symptoms become progressive and not responsive to aggressive conservative care, surgical options are available. Although hip fusion is one option, total hip replacement is the preferred surgical procedure. Total hip replacement makes dramatic improvements in quality of life for patients who need it. Total hip replacements can be done using cement or cementless techniques. Hybrid procedures using both cementless and cemented
parts are also available. In general, younger patients with healthy bones are offered the cementless replacements. Older patients, or patients with weak bones or rheumatoid arthritis, are typically offered the cemented replacements. Of course, patients should have a full discussion of all the risks and benefits of the different prosthesis options with their surgeon.
parts are also available. In general, younger patients with healthy bones are offered the cementless replacements. Older patients, or patients with weak bones or rheumatoid arthritis, are typically offered the cemented replacements. Of course, patients should have a full discussion of all the risks and benefits of the different prosthesis options with their surgeon.
HIP LABRAL TEAR
Background
The labrum is a fibrocartilaginous ring structure that encompasses and deepens the acetabulum of the hip. It functions as an interface and cushioning structure between the femoral head and the acetabulum. Like other fibrocartilaginous structures, the labrum of the hip is subject to injury, which usually occurs from repetitive stress from high-impact activities. This injury is usually seen in runners and dancers.
Clinical Presentation
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


