Impairment of brain function caused by trauma. May be due to direct blow or impulsive (whiplash) force.
Transient neurological symptoms that may or may not involve loss of consciousness.
Normal neuroimaging studies.
Incidence 0.25-5/1000 player hours of exposure for most sports.
Professional jumps jockeys have the highest concussion rate of any sport.
The pathophysiology is unknown. Speculated to affect the permeability and function of cell membranes within specific parts of brain or brainstem, which results in transient functional disruption.
Subtypes
There is no scientifically valid classification of concussion at the present time.
The majority (90-95%) of sports concussions recover in 7-10 days if managed appropriately. A small group of patients take longer to recover or have persistent symptoms and need expert multi-disciplinary management. In this chapter, these will be described as “complex” concussions.
Diagnosis is based on the presence of acute signs, symptoms, and cognitive impairment.
Symptoms
For symptoms of sports concussion, see Table 15.1.
Table 15.1 Symptoms of sports concussion
Symptoms
Signs
Cognitive
Headache
Loss of consciousness
Disorientation
Dizziness
Poor balance
Confusion
Nausea
Concussive convulsion
Amnesia
Unsteadiness
Vomiting
Easily distracted
‘Foggy’ or ‘dazed’
Slurred speech
Poor concentration
Ringing in the ears
Personality changes
Slow to answer questions
Double vision
Inappropriate playing behaviour
History and examination
Key features on history include: time and place of injury, mechanism of injury (eyewitness or video), presence, or duration of loss of consciousness (LOC), post-injury behaviour, presence of convulsions post-injury, past medical history, medication use, drug, and alcohol history.
Physical exam centres on the exclusion of intracranial pathology (e.g. haemorrhage) by neurological examination. A baseline GCS should be recorded. In sports concussion, there may be balance abnormalities within the first 72h of injury otherwise the physical exam is usually normal.
Key symptoms to flag
These signs and symptoms may indicate an intra-cerebral injury requiring urgent medical assessment. Err on the side of caution—‘If in doubt, check it out’.
A deterioration in the level of consciousness following injury.
Skull fracture.
Penetrating skull trauma.
Focal neurological symptoms or signs.
Loss of consciousness >5min.
Persistent vomiting or headache after injury.
Difficulty in assessing the patient due to alcohol, drugs, epilepsy, etc.
Other high-risk medical conditions (e.g. haemophilia).
The lack of a responsible adult to supervise the athlete post-injury.
More than one concussion in a match or training session.
Head injuries in children.
Diagnostic tests
Brain CT (or where available MR brain scan) contributes little to concussion evaluation, but should be employed if you suspect an intra-cerebral structural lesion.
Genetic testing
ApoE4 is one of a number of proposed genetic risk factors for adverse outcome following all levels of brain injury. The significance of ApoE4 in the risk of sports concussion or injury outcome is unclear.
Pre-participation physical examination
A detailed concussion and head injury (e.g. facial fractures) history is of value, but many athletes will not recognize or remember all concussions suffered in the past.
Convulsive and motor phenomena
A variety of acute motor phenomena (e.g. tonic posturing) or convulsive movements may accompany a concussion. Although dramatic, these clinical features are generally benign and require no specific management beyond the standard treatment for the underlying concussive injury. Because of the unusual and infrequent nature of this complication, it is recommended that they be managed as for a ‘complex’ concussion.
Second impact syndrome
Diffuse cerebral swelling is a rare but well recognized complication of mild traumatic brain injury that occurs predominantly in children and teenagers. Although repeated concussive injuries are proposed as the basis for this syndrome, a single impact of any severity may cause this rare complication.
Prevention of head injury
There is no clinical evidence that currently available protective equipment will prevent concussion. Protective equipment may prevent other forms of head injury, which may be important for those sports. However, remember the concept of risk compensation. This is where protective equipment results in behavioural change, including more dangerous playing techniques, with a paradoxical increase in injury rate.
Education
Athletes and their health care providers must be aware how to detect concussion, its clinical features, assessment techniques, and principles of safe return to play. Athletes particularly need to understand the significance and importance of concussion symptoms, and be able to discuss these with their doctor in a team environment, where there is no pressure to return to play prematurely.
Long-term problems
Other than the longstanding research of professional boxers and chronic brain injury, there are a number of lines of research highlighting concern over long-term sequelae of concussion in professional athletes. At this time, the incidence, risk factors, and prognosis for such problems is unknown.
Recent case reports have described the pathological findings of three cases of chronic traumatic encephalopathy (CTE) in retired professional American footballers and in a further line of epidemiological research looking at neurological problems in retired athletes, data suggests that the incidence of amyotrophic lateral sclerosis may be increased in association with head injury. There may be an as yet unknown genetic basis for this risk.
A separate cross-sectional study of 2552 retired professional NFL American footballers has identified an association between recurrent concussion and clinically diagnosed mild cognitive impairment, as well as self-reported significant memory impairments. In the same cohort, the authors found that 11.1% of all respondents reported having clinical depression. There was an association between recurrent concussion and diagnosis of lifetime depression, suggesting that the prevalence increases with increasing concussion history.
What is becoming increasingly clear from a number of diverse lines of research is that a small percentage of athletes seem to disproportionately suffer chronic or long-term sequelae from sports-related head injury. Interestingly, this does not seem to be confined to the brain, but affects the spinal cord and other parts of the nervous system. At this stage, very little is known about what type, frequency, or amount of trauma is necessary to induce the accumulation of these pathological tau proteins and more importantly why only a small number of athletes are at risk for CTE.
Management of sports concussion
Acute concussion management
When a player shows any symptoms or signs of a concussion:
The player should not be allowed to return to play in the current game or practice.
The player should not be left alone; and regular monitoring for deterioration is essential over the initial few hours following injury.
The player should be medically evaluated following the injury.
Return to play must follow a medically supervised stepwise process.
A player should never return to play or training while symptomatic. ‘When in doubt, sit them out!’
Sideline evaluation
Sideline evaluation of cognitive function is an essential component in the assessment of this injury. Brief neuropsychological test batteries such as the Maddocks questions, Standardized Concussion Assessment Tool 2 (SCAT2) or the Standardized Assessment of Concussion (SAC) have been validated in this setting. Internationally, the SCAT2 tool is the most widely used medical assessment tool and was developed at the 2009 Zurich expert consensus conference. The SCAT2 also has the Maddocks questions, GCS and SAC embedded within the tool. There is also a ‘Pocket SCAT2’ version for lay or non-medical assessment.
Standard orientation questions (e.g. time, place, person) are unreliable in the sporting situation compared with memory assessment.
Maddocks questions
The Maddocks questions are a validated brief assessment paradigm that can be easily administered on a sporting field or on the sidelines. They are also included in the SCAT2 tool. Failure to answer all questions correctly should raise suspicion of a concussive injury.
Which ground are we at?
Which team are we playing today?
Who is your opponent at present?
Which quarter is it?
How far into the quarter is it?
Which side scored the last goal?
Which team did we play last week?
Did we win last week?
Sideline assessment of cervical spine injury
Think cervical spine injury, always! If an alert patient complains of neck pain, has evidence of neck tenderness or deformity, or has neurological signs suggestive of a spinal injury, then neck bracing and transport on a suitable spinal frame is essential. If the patient is unconscious, then a cervical injury should be assumed until proven otherwise. Airway protection takes precedence over any potential spinal injury. In this situation, the removal of helmets or other head protectors should only be performed by individuals trained in this aspect of trauma management.
Concussion injury severity grading
International expert consensus has abandoned anecdotal grading scales in favour of combined measures (clinical symptoms, physical exam, cognitive assessment) of recovery in order to determine injury severity and, hence, guide return to play decisions. There is limited published evidence that concussion injury severity correlates with the number and duration of acute concussion signs and symptoms and/or degree of impairment on neuropsychological testing.
Neuropsychological assessment post-concussion
Neuropsychological (NP) testing in concussion is of value and continues to contribute significant information in concussion evaluation. NP assessment should not, however, be the sole influence on the decision to return to play, but is an aid to clinical decision making. NP test batteries are most useful with baseline pre-injury testing and serial follow-up post-injury. NP assessment is problematic in under 15 years of age due to changing baselines reflecting cognitive maturation. In this age group, paediatric NP expertise may be required in some cases for a full assessment.
Post-concussion balance assessment
Balance testing, either with computerized platforms or clinical assessment (e.g. BESS scale), may offer additional important information particularly in the first 72h following injury. A balance assessment is incorporated in the SCAT2.
Return to play (RTP) protocol
The vast majority of injuries are uncomplicated or simple concussions that recover spontaneously over 7-10 days and an athlete usually proceeds rapidly through the stepwise return to play strategy. During the first few days following an injury, it is important to emphasize to the athlete that physical and cognitive rest is required. Activities that require concentration and attention (such as videogames) may exacerbate the cognitive symptoms and as a result delay recovery.
Return to play follows a stepwise process:
Step 1: no activity, complete rest. Once asymptomatic, proceed to next level.
Step 2: light aerobic exercise, such as walking or stationary cycling, no resistance training.
Step 3: sport-specific training (e.g. skating in hockey, running in soccer), progressive addition of resistance training at steps 3 or 4.
Step 4: non-contact training drills.
Step 5: full contact training after medical clearance.
Step 6: game play.
If any post-concussion symptoms occur, the patient should drop back to the previous asymptomatic level and try to progress again after 24h. In cases with persistent symptoms beyond 10 days, the rehabilitation will be more prolonged and return to play advice will be more circumspect. Such complex cases should be managed by physicians with specific expertise usually in a multidisciplinary setting.
Concussed athletes should not only be symptom free, but should not be taking any pharmacological agents/medications that may affect or modify the symptoms of concussion prior to consideration of RTP.
The Standardized Concussion Assessment Tool 2 card cognitive screen in concussion
The SCAT is a medical assessment card that may be used in the assessment of concussed athletes. The original version was developed in 2005 and then revised (called the SCAT2) following scientific studies at the 2009 Zurich international consensus meeting. In addition to symptom assessment, cognition and physical exam, the tool incorporates the Maddocks questions, GCS, and the SAC, and is designed to be used by medical staff. A shorter version designed to be used by lay or non-medical personnel (called the ‘PocketSCAT2’) was developed at the same time and enables the user to suspect the diagnosis of concussion and refer the patient for medical assessment.
Glasgow Coma Scale
The most widely used traumatic brain injury severity scale throughout the world is the Glasgow Coma Scale (GCS). It is useful in categorizing the acute injury, mild, moderate, and severe injuries, and performed serially to monitor progress over time. Deterioration in the GCS score may herald intracranial complications requiring neurosurgical or neuro-intensive care intervention (see Table 15.2).
Table 15.2 The Glasgow Coma Scale
Category
Response
Score
Eye opening response (E)
Spontaneous
4
To speech
3
To pain
2
No response
1
Verbal response (V)
Orientated
5
Confused, disorientated
4
Inappropriate words
3
Incomprehensible sounds
2
No response
1
Motor response (M)
Obeys commands
6
Localizes
5
Withdraws (flexion)
4
Abnormal flexion (posturing)
3
Extension (posturing)
2
No response
1
Reproduced from Teasdale, G. and Jennett, B., Lancet, 304: 7872 (1974), with kind permission from Elsevier
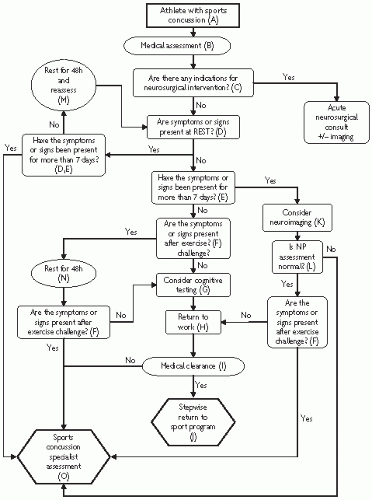
Flow chart
The flowchart (Fig. 15.1) is a conceptual management approach to provide advice regarding return to work and sport. At least 7 days should have passed in order to detect resolution of symptoms. In the first 7 days there are currently no prognostic means of separating simple and complex concussive injury. There is still, therefore, an important role for physician discretion in neuroimaging and/or neuropsychological assessment in this early period. This management algorithm provides general guidance only. The letters in parentheses correspond to the flowchart:
(A) This refers to athletes with no evidence of previous concussion and no history of behavioural, neurological, psychological problems, or learning disorder. Any return to sport also presumes that the athlete is free of any drugs, alcohol, or medication that may mask symptoms or interfere with cognitive performance.
Fig. 15.1 Sports concussion algorithm.
(B) Initial medical assessment involves history, neurological exam, physical exam including examination of face, skull, and cervical spine and SCAT card assessment.
(C) Indications for neurosurgical intervention are detailed elsewhere.
(D) Symptoms and signs of concussion are presented in Table 15.1.
(E) The Prague guidelines allow 7-10 days for symptoms and signs of simple concussion to resolve. Until this timeframe is formally validated in athletes, we recommend 7 days, although recognize that physician discretion should apply.
(F) An exercise challenge requires the athlete to exercise until heart rate is greater than 60% of maximum predicted heart rate (MPHR). MPHR = 220 – age in years. As a simple ‘rule of thumb’ this corresponds to a heart rate of >120beats/min.
(G) Formal neuropsychological testing is not required for simple concussion. However, the athlete must be able to score normally on the SCAT card mental status assessment. If this assessment is abnormal then more formal neuropsychological assessment may be warranted.
(H) Return to work or school is dependent upon complete resolution of symptoms, signs, and cognitive function both at rest and after exercise. Athletes should be medically reassessed after return to work or school to ensure functional recovery before proceeding to the stepwise return to play guideline. When considering return to school, it would be prudent for the teachers and parents to be aware of potential problems that may arise at this stage.
Only gold members can continue reading. Log In or Register to continue