In 1934, Codman (1) coined the term frozen shoulder and described it as a “condition difficult to define, difficult to treat, and difficult to explain from the point of view of pathology.” Adhesive capsulitis has continued to be one of the most poorly understood disorders of shoulder, posing significant challenges to the clinician. Much of the problem stems from the fact that it has not been easy to define or clearly differentiate from conditions with similar symptoms and findings but with distinctly different causes.
CLASSIFICATION AND DEFINITION
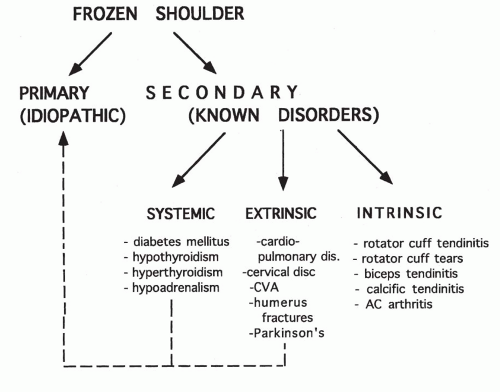
Numerous classification systems have been proposed, with a loosely woven common thread of the presence or absence of trauma (2, 3, 4, 5, 6). Reeves (5) used the subgroupings “idiopathic frozen shoulder” and “posttraumatic stiff shoulder” and related his arthrographic findings to the clinical descriptions provided by Jones and Lovett (7). Lundberg (8) classified patients with this condition into two groups: primary or secondary frozen shoulders. Primary frozen shoulder represents the idiopathic condition; secondary frozen shoulder is associated with a known intrinsic, extrinsic, or systemic abnormality. Although this is a worthwhile distinction, it is probably inappropriate to group all intrinsic, extrinsic, and systemic causes as secondary frozen shoulder. Extrinsic conditions such as cervical spine and intrathoracic disorders and systemic conditions such as diabetes mellitus should be considered together. Intrinsic disorders such as rotator cuff injury should be considered separately because they represent a known underlying primary disorder that results in the clinical picture of frozen shoulder (9). This schema is shown in Figure 8-1.
In addition to numerous classifications, the definition of frozen shoulder has varied greatly in the literature. In the late 19th century, Duplay in France (10) and, soon after, Putnam in North America (11) described “scapulohumeral periarthritis,” which encompassed a broad spectrum of pathologic conditions causing similar symptoms of painful shoulder stiffness and dysfunction. In 1945, Neviaser (12) proposed the term “adhesive capsulitis,” which he believed better described the underlying pathology. He identified a “chronic inflammatory process involving the capsule of the shoulder causing a thickening and contracture of this structure which secondarily becomes adherent to the humeral head.” Today, this term is often used synonymously with frozen shoulder and, unfortunately, is also commonly used as an incorrect synonym for stiffness occurring secondary to an inciting event.
The senior author polled members of the American Shoulder and Elbow Surgeons (ASES) to ensure the best consensus on the definition of frozen shoulder, defining it as “a condition of uncertain etiology characterized by significant restriction of both active and passive shoulder motion that occurs in the absence of a known intrinsic shoulder disorder.”
EPIDEMIOLOGY
Although the exact prevalence and incidence of frozen shoulder are unknown, most studies report the cumulative risk for at least one episode to be 2% (8). It is most frequently found in patients between the fourth and sixth decades of life, and it is more common in women than men (13). The nondominant extremity seems to be more commonly involved, with most reported cases describing an affected left side (8,14,15). Bilateral involvement occurs in 6% to 50% of cases, although only 14% of these bilateral cases manifest simultaneously (8,13,16, 17, 18). When a history of bilateral involvement is identified, the possibility of a constitutional predisposition should be explored (8,19,20).
Figure 8-1 Proposed pathways for the development of frozen shoulder syndrome. (Reprinted from Warner JJP, Iannotti JP, Flatow EL, eds. Complex and Revision Problems in Shoulder Surgery, 2nd ed. Philadelphia: Lippincott Williams & Wilkins, 2005:206, with permission.)
PATHOGENESIS
Different pathologic mechanisms have been proposed to explain the cause of frozen shoulder, but all remain largely theoretic. The most common theories are reviewed here. Many plausible pathogenic mechanisms have been proposed during the last 60 years, yet none of the factors occasionally isolated and associated with the pathogenesis of frozen shoulder have been consistently found (Table 8-1) (21).
Several investigators have proposed an autoimmune basis for frozen shoulder (16,17,22, 23, 24). Although some clinicians have reported a high incidence of human leukocyte antigen (HLA) B27 in patients with frozen shoulder (22), others have not confirmed this association (25, 26, 27, 28). In later studies, serum immunoglobulin (Ig) A levels were found to be significantly lower in patients with frozen shoulder, and immune complex and C-reactive protein levels were increased (16,17,23). In general, however, sufficient evidence to support an immunologic theory has been lacking.
A biochemical basis for frozen shoulder has also been proposed. In his analysis of the capsule in patients with frozen shoulder, Lundberg (8,29) found an increase in glycosaminoglycan and a decrease in glycoprotein content. These biochemical changes in the capsule, however, are consistent with the process of fibrosis, and they may represent the effect of frozen shoulder rather than its cause.
Neurologic dysfunction has been postulated to be a cause of frozen shoulder. In 1959, Kopell (30) proposed suprascapular compression neuropathy as a possible cause of frozen shoulder, but electromyography and nerve conduction studies have not supported this theory. Others have suggested that frozen shoulder is a result of autonomic dysfunction and represents a form of reflex sympathetic dystrophy (20). However, sufficient evidence to support these hypotheses has not been provided.
Various endocrine disorders are associated with frozen shoulder. Patients with diabetes mellitus in particular manifest a much greater incidence of frozen shoulder than nondiabetic controls. Bridgman (31) found that the incidence of frozen shoulder in 800 diabetic patients was 10.8%, compared with 2.3% in 600 nondiabetic controls. Another study identified abnormal glucose tolerance test results for 28% of patients with frozen shoulder, compared with 12% in age- and sex-matched controls with other rheumatologic conditions (32). Frozen shoulder has also been reported to occur with increased incidence among patients with thyroid disorders (33,34) as well as those with hypoadrenalism (35) or corticotropin deficiency (36).
Trivial trauma has been postulated to be an important factor, particularly when it is followed by a period of immobilization (37,38). This does seem to be the sequence of events in some patients who develop frozen shoulder (20). However, most patients who sustain minimal trauma, even when combined with a period of immobilization, do not develop frozen shoulder. This has led some investigators to conclude that there are some patients who possess a “constitutional predisposition” for the development of frozen shoulder. Support for this theory is provided by the significant incidence of bilateral frozen shoulders (8,18,22,39,40).
TABLE 8-1 PROPOSED PATHOGENIC MECHANISMS FOR PRIMARY FROZEN SHOULDER
Mechanism
Disorder
Pathology
Etiology Excluded By
Autoimmune
Collagen-vascular disorders
Type IV reaction (to infarcted cuff tendon)
Absence of immune complexes and autoantibodies, no other affected joints
Inflammatory
Infectious arthritis
Vital, bacterial, or fungal infection
Absence of prodromal illness and systemic symptoms
Crystal arthropathy
Calcium pyrophosphate dihydrate disease and gout
Crystal deposition
Absence of recurrences, crystals, and inflammatory phases
Reactive arthropathy
Spondyloarthritides and ankylosing spondylitis
Seronegative arthritis
No systemic manifestations, normal joint fluid, no blood markers
Hemarthrosis
Hemoglobinopathies and trauma
Chemical irritation (hemosiderin)
No capsulitis or fibrositis with hemoglobinopathies
Paralytic
Suprascapular nerve palsy
Compression neuropathy
Absence of electromyelogram or conduction abnormalities
Algodystrophy
Autonomic neuropathy
Neuropatic disturbance and hypervascularity
No sensory or vascular deficiency, stellate ganglion block not helpful
Degenerative
Rotator cuff tendon and degeneration/infarctoin
Microvascular infarction
Absence of tendon inflammation of infarction
Traumatic
Trauma and immobilization
Injury synovitis and tissue contracture
Brief shoulder stiffness after prolonged casting in the majority
Psychogenic
Hysteria and hypochondriasis
Depression, dependence, and chronic pain disorder
Similar Minnesota Multiphasic Personality Inventory between patients and controls
Fibrogenic
Cytokine induction of fibroplasia
Tissue contracture in response to cytokines, inflammatory cell products, and platelet-derived growth factor.
Represents only one phase of the disease
From Harryma DT II. Shoulders: frozen and stiff. Instr Course Lect 1993;42:247-257.
The role of psychologic factors has been considered in the development of frozen shoulder. Some investigators have suggested that a certain personality structure, coupled with untoward life events and inappropriate responses to stress, may serve as a predisposing or precipitating factor for the development of frozen shoulder (20,41, 42, 43). Other studies, however, have found no evidence for a characteristic personality disorder (39,40).
It appears that the precise cause for the development of frozen shoulder remains largely unknown. The condition probably results from the proper combination of host factors (i.e., predisposition) and extrinsic factors (e.g., trauma, hormonal changes, collagen-vascular disease, diabetes mellitus).
PATHOLOGY
Several investigators have described the pathologic findings associated with frozen shoulder in an attempt to offer an explanation for the observed macroscopic capsular changes (1,8,44, 45, 46, 47, 48, 49, 50, 51). Neviaser (48) coined the term adhesive capsulitis to describe an “avascular, tense capsular markedly adherent to the humeral head and associated with a decreased joint volume and synovial fluid.” The histologic changes were consistent with chronic inflammation, fibrosis, and perivascular infiltration in the subsynovial layer, with the synovial layer remaining uninvolved (48).
Based on intraoperative findings of gross contracture of the rotator cuff, Macnab (44) postulated that the primary lesion was in the cuff itself, with subsequent contracture in the capsule and coracohumeral ligament. He confirmed a region of constant hypovascularity in the supraspinatus tendon, called the critical zone by Codman (1), and theorized that this was responsible for the initial cuff degeneration (50). Ozaki and associates (49) described the role of contracture of the coracohumeral ligament and the rotator interval in the pathogenesis of frozen shoulder. These investigators found fibrosis, hyalinization, and fibrinoid degeneration in these structures. Neer (47,52) also reported the importance of the coracohumeral ligament contracture, but he stressed that it was unlikely that any one anatomic structure or pathologic process was responsible for causing the entire symptom complex associated with frozen shoulder.
An association between clinical frozen shoulder and Dupuytren’s contracture has been identified by multiple authors dating back to 1936 (53). Biopsy samples of the rotator interval and coracohumeral ligament in patients with idiopathic frozen shoulder have demonstrated active fibroblastic proliferation amidst thick nodular bands of collagen accompanied by some transformation to a smooth muscle phenotype (myofibroblasts) very similar to the fibrotic changes seen in Dupytren’s disease of the hand (54). These findings reflect at least one phase (i.e., freezing phase) of frozen shoulder (55).
Rodeo and associates (56) compared capsular tissue samples from patients with adhesive capsulitis and controls to determine specific cytokines involved in the inflammatory and fibroblastic response. Transforming growth factor (TGF)-β, platelet-derived growth factor (PDGF), and hepatocyte growth factor (HGF) are involved in the early inflammatory stages of adhesive capsulitis. PDGF is a mitogenic agent that causes fibroblastic cell proliferation and TGF-β increases extracellular matrix, both being potential precursors of capsular fibrosis. These findings are supported by Suzuki et al. (57) who found that PDGF-AB, HGF, and insulin-like growth factor type I all stimulated the migration of fibroblasts. Hannafin et al. (58) hypothesized that the hypervascular synovitis seen in adhesive capsulitis, via cell-mediated pathways, provokes a progressive fibroblastic response in the adjacent capsule resulting in diffuse capsular fibroplasia, thickening, and contracture. Recently, matrix metalloproteinases (MMPs), a family of naturally occurring proteinases, have been implicated as a contributing factor in the pathogenesis of frozen shoulder because they play a key role in controlling collagen matrix remodeling (59,60). Results from these studies suggest that although abnormalities in MMP expression are present in patients with frozen shoulder, a causal relationship cannot be established.
STAGING
Three distinct but overlapping phases with a variable clinical course of variable duration have been defined:
Painful phase characterized by insidious onset of diffuse pain lasting 2 to 9 months.
Stiffening or freezing phase characterized by progressive motion restriction lasting 4 to 12 months.
Thawing phase characterized by gradual resolution of pain and stiffness lasting up to 42 months.
Hannafin et al. (61) modified the traditional staging scheme incorporating clinical presentation, arthroscopic finding, and histological appearance of the capsular specimens:
Stage 1: Painful Phase
Duration: 0 to 3 months
Pain with active and passive range of motion (ROM)
With or without limitation of forward elevation (FE), abduction (Abd), internal rotation (IR), external rotation (ER)
Exam under anesthesia (EUA) or after glenohumeral (GH) injection: normal or minimal loss of motion
Arthroscopic findings: diffuse GH synovitis, most pronounced in the anterosuperior capsule
Stage 2: Freezing Phase
Duration: 3 to 9 months or more
Chronic pain with active and passive ROM
Significant limitation of FE, Abd, IR, ER
EUA or after GH injection: ROM under anesthesia/injection = ROM awake/no injection
Arthroscopic findings: diffuse pedunculated synovitis (tight capsule with rubbery or dense feel on insertion if the arthroscope)
Pathologic changes: hypertrophic, hypervascular synovitis with perivascular and subsynovial scar, fibroplasias and scar formation in underlying capsule
Stage 3: Frozen Phase
Duration: 9 to 14 months
Minimal pain except at end ROM
Significant limitation of ROM with rigid “end feel”
EUA or after GH injection: ROM under anesthesia/injection = ROM awake/no injection
Arthroscopic findings: no hypervascularity seen, remnants of fibrotic synovium can be seen. The capsule feels thick on insertion of the arthroscope with diminished capsular volume
Stage 4: Thawing Phase
Duration: 15 to 24 months
Minimal pain
Progressive improvement in ROM
EUA/arthroscopy: Data not available
SECONDARY FROZEN SHOULDER
Frozen shoulder associated with a known underlying disorder is considered to be secondary; this group includes intrinsic, extrinsic, or systemic disorders. Intrinsic shoulder abnormalities include rotator cuff tendonitis, rotator cuff tears, tendonitis of the long head of the biceps tendon, calcific tendonitis, and acromioclavicular (AC) arthritis. Extrinsic disorders, which represent pathologic conditions remote from the shoulder region, include: ischemic heart disease and myocardial infarction (40,62); pulmonary disorders including tuberculosis (63), chronic bronchitis, emphysema (64), and tumors (65); cervical disc disease and radiculopathy (13,40,66); cerebral vascular hemorrhage (67,68); previous coronary artery bypass graft surgery (69); previous breast surgery; lesions of the middle humerus (70); and central nervous system disorders such as Parkinson’s disease (71). Systemic disorders represent generalized medical conditions that are known to occur in association with frozen shoulder. Such conditions include diabetes mellitus, hypothyroidism, hyperthyroidism, and hypoadrenalism.
POSTSURGICAL STIFFNESS
Surgical procedures in the shoulder are widely recognized as a cause of shoulder stiffness. These include: capsular procedures (i.e., capsulorrhaphies, open inferior capsular shifts), rotator cuff repairs (open and arthroscopic), labral repairs, and proximal humerus fractures. Surgical procedures in the vicinity of the shoulder include axillary node and cervical neck dissection, cardiac catherization in the axilla, coronary artery bypass grafting with sternotomy, and thoracotomy. Differentiation between primary adhesive capsulitis and postsurgical stiffness is usually made by the history. Primary adhesive capsulitis results in more global restriction of motion, whereas postsurgical stiffness can result in more selective restriction depending on which structures were tightened.
CLINICAL PRESENTATION
Patient History
Because frozen shoulder represents a symptom complex rather than a specific diagnostic entity, a careful clinical history is crucial in making the diagnosis. Patients with this condition report a gradual loss of function associated with vague discomfort about the shoulder after minimal or no trauma at all. These symptoms, which often are worse at night, usually begin insidiously. Overhead and behind-theback activities become especially difficult to perform as motion is diminished. These symptoms closely resemble those found in patients with rotator cuff problems, thereby requiring a careful physical examination to consider frozen shoulder as the primary condition or one that is secondary to a specific shoulder problem.
Physical Examination
Physical examination of the cervical spine, opposite shoulder, and trunk should always be performed to exclude any associated abnormality. The clinical hallmark is the limitation of active and passive range of glenohumeral motion. The degree of motion, including FE in the scapular plane, ER at 0 degrees adduction, and IR relative to the spinous process must be documented accurately. Pain (depending on the stage) may be absent when the shoulder is moved within its free range (47). A firm endpoint is appreciated, with pain at the extremes of motion. There has been little consensus about the degree of restriction of shoulder motion needed to make a diagnosis of frozen shoulder (16,17). In general, ER, abduction, and IR are the motions that are most affected, with mild restriction in ER as the most sensitive early indicator (68). Unless there is associated rotator cuff tendonitis, strength tested in the midrange is usually unaffected.
LABORATORY AND IMAGING STUDIES
Routine hematologic testing should include a complete blood cell count, chemistry profile, rheumatoid factor test, and serology, even though the results are usually normal. The erythrocyte sedimentation rate is elevated in as many as 20% of patients (16,17). Except for osteopenia associated with disuse, radiographic findings are usually negative. Significant findings, however, may aid in the identification of an underlying intrinsic disorder, and a complete set of radiographs consisting of anteroposterior (in neutral, internal, and external rotation), supraspinatus outlet, and axillary views should be obtained.
Technetium bone scanning has been used in the evaluation of frozen shoulder. Findings of increased uptake, although nonspecific, are probably secondary to hypervascularity. Such studies have not been shown to have any correlation with disease symptoms, duration, or prognosis (17,72).
Arthrography (18,27,73, 74, 75, 76, 77, 78) for the diagnosis of frozen shoulder is of historic interest. Typical findings associated with frozen shoulder include a reduced joint volume (5 to 10 mL), obliteration of the axillary recess and subscapularis bursa, and absence of contrast in the biceps tendon sheath (67,73,79). Such findings, however, have not been shown to have any predictive value in terms of disease severity or prognosis (72,77,80). The use of magnetic resonance imaging (MRI) in the diagnosis of frozen shoulder is equivocal with some studies documenting increased capsular thickness and synovial enhancement (81). MRI is most useful in ruling out associated intrinsic shoulder abnormalities (i.e., rotator cuff tendonitis, rotator cuff tears, tendonitis of the long head of the biceps tendon and calcific tendonitis, glenohumeral arthrosis, and AC arthrosis).
Only gold members can continue reading. Log In or Register to continue
 Complications of Surgery to the Acromioclavicular and Sternoclavicular Joints
Complications of Surgery to the Acromioclavicular and Sternoclavicular Joints
 Neurologic Injury
Neurologic Injury
 Complications of Glenohumeral Arthrodesis
Complications of Glenohumeral Arthrodesis
 Arthroscopy: Complications of Surgery for Instability
Arthroscopy: Complications of Surgery for Instability
 Arthroscopy: Complications of Rotator Cuff Repair
Arthroscopy: Complications of Rotator Cuff Repair
 Complications of Arthroscopic Subacromial Decompression and Acromioclavicular Joint Resection
Complications of Arthroscopic Subacromial Decompression and Acromioclavicular Joint Resection



