Fractures Of The Forearm And Distal Radius
David V. Lopez
Robert L. Kalb
The forearm consists of the radius and ulna shafts. Maintaining their anatomic relationship preserves pronation and supination. As a result, many fractures of the forearm require operative fixation. Also mentioned here are injuries to the distal radius.
FOREARM FRACTURES
Mechanism of Injury
A direct injury or a fall on an outstretched arm may precipitate an injury.
Diagnosis
Forearm fractures are associated with swelling, pain, and point tenderness. Neurovascular structures are intimately associated with the osseous structures in this area; a careful examination is important.
Radiology
Plain anteroposterior and lateral radiographs provide sufficient information for diagnosis and management (Fig. 1). There may be an isolated or both-bone fracture of the radius and ulna. The Monteggia fracture (Fig. 2) is a fracture of the proximal ulna with dislocation of the radial head. The Galeazzi fracture (Fig. 3) is a fracture of the distal third of the radius with dislocation or subluxation of the distal radioulnar joint.
Initial Treatment
With the exception of the isolated ulna fracture (nightstick fracture), all of these injuries are best immobilized using a long-arm posterior splint. Traction in fingertraps may be necessary to correct angulation. Isolated ulna shaft fractures with less than 50% displacement and 15 degrees of angulation may be managed nonoperatively. A long-arm posterior splint may be applied.
Definitive Treatment
The splint is changed to a cast for a total of 8 weeks of immobilization.
When to Refer
All forearm injuries except for the isolated ulna shaft fracture should be referred within 1 week for possible operative treatment.
Complications
In evaluating patients with forearm fractures, one should be cognizant of compartment syndrome. This is increased pressure within the nonexpandable volar forearm compartment. It is characterized by the five Ps: pain, paresthesias, pressure, pallor, and pulselessness. The earliest and most reliable symptom is pain out of proportion to the injury. The earliest sign is hypoesthesia to light touch in the median nerve distribution (volar thumb). Another
early sign is pain with passive thumb extension. A compartment syndrome is a surgical emergency requiring fasciotomy and, once suspected, should be emergently referred. Also, immediately remove the cast and Webril.
early sign is pain with passive thumb extension. A compartment syndrome is a surgical emergency requiring fasciotomy and, once suspected, should be emergently referred. Also, immediately remove the cast and Webril.
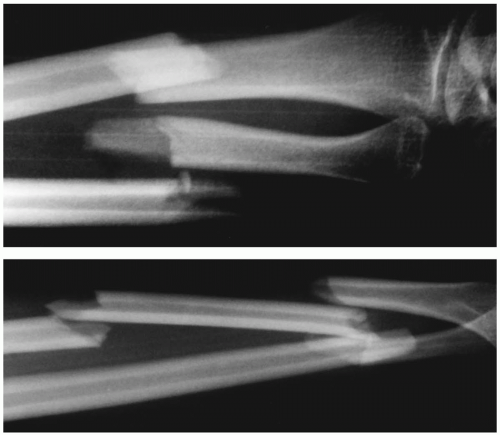 Figure 1 Displaced fractures of both bones of the forearm in a 34-year-old woman as a result of a motor vehicle accident. The radial fracture was segmental. |
DISTAL RADIUS FRACTURES
Mechanism of Injury
This injury is very common in the elderly and osteoporotic populations. Most often, one falls on an outstretched hand.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


