Foot Fractures
Arthur W. Pallotta
Robert L. Kalb
TALUS FRACTURES
During the Second World War, the foot controls of airplane landing gear were mechanical. Sometimes, these controls would snap back suddenly into the sole of the foot of the pilot, resulting in axial loading of the talus and a fracture. During that time, the talus fracture became known as aviator’s astragalus (Fig. 1).
Mechanism of Injury
The talus can fracture with a sudden axial loading on the foot, most commonly with dorsiflexion (Fig. 2).
Diagnosis
The symptoms of talus fracture are similar to those of an ankle fracture.
Radiology
Anteroposterior (AP), lateral, and oblique views of the foot should be obtained along with AP, lateral, and mortise (discussed in Chapter 10) views of the ankle.
Initial Treatment
Emergent treatment is instrumental in preserving neurologic and vascular function. If dislocation is present, an immediate reduction is indicated. If the dislocation cannot be reduced, emergent open reduction is indicated to decrease the chance of avascular necrosis.
Definitive Treatment
The definitive goal is to obtain the best possible reduction and to protect the reduction. This gives the best chance at union and reduces the incidence of posttraumatic arthritis. The risk of avascular necrosis is proportional to the original amount of displacement. If the fracture is nondisplaced, use a short-leg cast for 6 weeks, non-weight bearing, followed by an additional 6 weeks of weight bearing in the cast.
When to Refer
Any talus fracture that is displaced should be seen by an orthopedist that day.
Complications
Patients should be informed that there is a high incidence of osteoarthritis, as well as avascular necrosis. Talus fracture complications are as common as those in the scaphoid.
CALCANEUS FRACTURES
The most common mechanism for calcaneus fracture (axial loading) often produces concomitant thoracic and lumbar compression fractures.
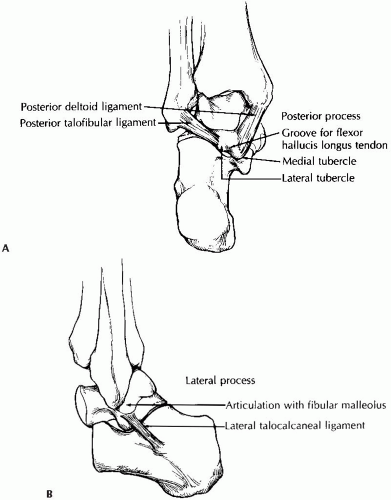 Figure 1 A: The posterior process of the talus has two tubercles, which are separated by the groove for the flexor hallucis longus tendon. The posterior fibers of the deltoid ligament insert into the medial tubercle, and the posterior talofibular ligament inserts into the lateral tubercle. B: The lateral process of the talus. |
Mechanism of Injury
The calcaneus can be fractured as a result of a fall from a height, jumpers’ injuries, or a direct blow striking the posterior calcaneus.
Diagnosis
History of fall from a height with pain in the heel or tenderness over the medial, lateral, or plantar surface of the calcaneus should raise suspicion. It is usually accompanied by ecchymosis, swelling, and pain with weight bearing. Palpate thoracic and lumbar spinous processes for associated injuries.
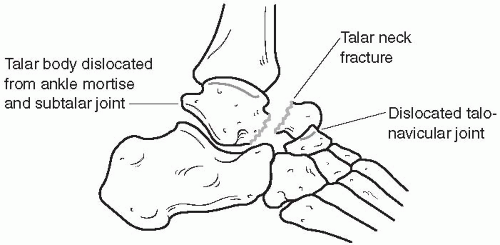 Figure 2 Talar neck fracture. Note that, in addition to the displacement of the talar body with subluxation of the subtalar joint, the talonavicular joint is also dislocated. |
Radiology
AP, lateral, and oblique views of the foot should be obtained, as well as an axial view of the calcaneus (Fig. 3). Computed tomography is often necessary to evaluate the articular surfaces. Thoracic and lumbar spine films to aid in ruling out associated compression fractures should be done if tenderness is noted.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


