Foot
Fracture of the calcaneus
History and examination
Acute fractures usually occur as the result of a fall from a height and are therefore uncommon in sports.
Investigation
X-ray.
Treatment
Generally treated conservatively with a period of bed rest in the acute stage, followed by non-weight bearing on crutches, progressing to full weight bearing as tolerated.
Fractures of the anterior process of the calcaneus can complicate an acute ankle sprain and, if displaced, may require open reduction and internal fixation.
Fracture of the metatarsal bones
History and examination
Fractures occur commonly in many sports.
May be caused by direct trauma (e.g. a kick in football) or a twisting injury (usually resulting in a spiral fracture).
Avulsion fractures of the base of the 5th metatarsal may complicate acute ankle sprains.
See also Jones fracture of the 5th metatarsal (p. 701).
See Fig. 24.1 for anatomy of the tarsal bones.
Investigation
X-ray.
Treatment
Generally respond well to conservative measures—strapping or use of a walking cast for a period of two or three weeks, followed by a return to sport in approximately six to eight weeks.
Complications are rare—see Jones fracture of base of 5th metatarsal.
Fitness should be maintained through non-weight-bearing activities, such as cycling, aqua jogging, or swimming.
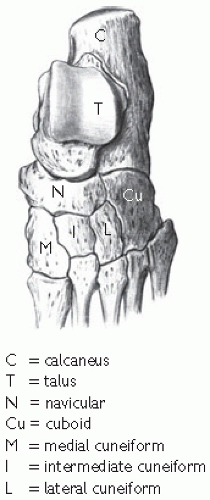 Fig. 24.1 Tarsal bones: dorsal view. Reproduced with permission from MacKinnon P and Morris J. (2005). Oxford Textbook of Functional Anatomy, Vol. 1. Oxford University Press, Oxford. © 2005. |
Lisfranc fracture: dislocations
History and examination
Occurs at the tarsometatarsal joints and are rare in sports.
Usually occur as the result of an acute plantar flexion injury.
Investigations
Plain X-ray appearances are subtle and may be missed. Weight-bearing views may demonstrate a diastasis between the first and second metatarsal bases, and occasionally a bone fragment may be present.
Treatment
Aimed at restoring the exact anatomical alignment and may be conservative for minor (grade 1 and 2 sprains) injuries or pinning of more severe, unstable injuries.
Return to sport following these injuries is prolonged—often up to 1 year.
Fat pad contusion
History and examination
Occurs either as a result of landing from a jump directly onto the heel, or due to repetitive heel strike on hard surfaces (especially in heavy individuals or those wearing inadequate footwear).
Fat pad atrophy may be precipitated by steroid injection (e.g. for plantar fasciitis) and is irreversible.
Tenderness is felt more proximally than with plantar fasciitis.
Investigations
Not necessary.
Diagnosis based on clinical findings.
Treatment
Includes the use of shock-absorbing heel cushions, taping, and modification of training surfaces.
Footwear with a firm heel counter should be worn to prevent splaying of the heel pad.
Midtarsal joint sprains
History and examination
Sprains may occur as a result of an acute injury or due to repetitive stress in an individual with an over pronated gait. They generally involve the calcaneonavicular ligament.
Investigations
Diagnosis based on clinical findings.
X-ray may be undertaken to exclude other causes of mid-foot pain.
Treatment
Conservative treatment with electrotherapeutic modalities and taping/orthotic supports.
Occasionally a cortisone injection is required if there is a persistent synovitis of one of the midtarsal joints.
Turf toe
History and examination
An acute dorsiflexion sprain injury of the first metatarsophalangeal joint.
Common on artificial surfaces where traction between the surface and the shoe is great, the foot moves forward pushing the toe upwards.
Severe injuries may result in dislocation of the first metatarsophalangeal joint, but most are typical sprain injuries.
Investigation
X-ray to exclude a fracture.
Treatment
Managed conservatively with ice, analgesics, rest, and taping to limit joint movement on return to sport (generally after 2-4 weeks).
These injuries can result in persistent discomfort on return to running.
May result in the development of hallux limitus.
Choice of footwear is important in preventing these injuries, with a rigid insole limiting excessive movement at the first metatarsophalangeal joint (MTPJ) (especially in those with hallux limitus).
Hallux rigidus (footballer’s toe)
History and examination
Occurs after repeated minor injuries to the 1st MTPJ resulting in early degenerative changes and restricted movement, especially dorsiflexion.
Very common in sports such as soccer, where repetitive stress occurs during kicking and sprinting.
This condition may cause the athlete to change his normal gait pattern to push off on the lateral border of the forefoot rather than at the hallux.
Investigation
X-ray will show osteophyte formation and joint space narrowing.
Treatment
Very difficult: NSAIDs and corticosteroid injection may give temporary relief.
Referral to a podiatrist is indicated as orthotics may help unload the joint.
Surgery to remove the osteophytes in more severe cases.
The term hallux limitus is used to describe less severe cases of this condition.
Normal walking
The normal gait cycle consists of heel strike (usually towards the lateral border of the heel with the foot slightly supinated), stance phase and toe off with the gait cycle completed by the swing phase leading to heel strike once more.
During distance running this gait cycle is maintained.
In sprinting the stance phase tends to consist of a midfoot or forefoot rather than a heel strike (i.e. sprinters tend to run more on their toes).
Following heel strike, the foot pronates (see Fig. 24.2 to allow full contact with the ground, subsequently supinating to form a rigid lever to allow toe off to occur.
The subtalar joint is responsible for the conversion of the rotatory forces of the lower limb and is important in dissipating shock following foot strike. Stiffness of the subtalar joint will reduce the ability to absorb shock.
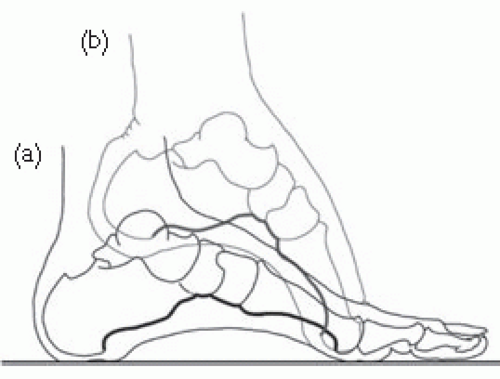 Fig. 24.2 (a) Medial longitudinal arch of the foot when standing. (b) Change in medial arch and dorsiflexion of metatarsophalangeal joint when standing on tip-toe and at the start of locomotion. Reproduced with permission from MacKinnon P and Morris J. (2005). Oxford Textbook of Functional Anatomy, Vol. 1. Oxford University Press, Oxford, © 2005. |
Pronation
Pronation is a tri-planar movement occurring at the subtalar joint.
Pronation is a normal component of the gait cycle.
Pronation consists of eversion, dorsiflexion, and abduction of the foot.
Pronation should not occur past the latter stages of midstance, as the normal foot should then supinate in preparation for toe off.
Excessive (over) pronation may contribute to, or be a consequence of, biomechanical anomalies elsewhere in the kinetic chain, placing abnormal stresses on other structures (e.g. will cause internal rotation of the lower limb and place abnormal stress on the medial structures of the foot and ankle).
Over pronation or hyperpronation has been implicated as a causative factor in the development of many lower limb problems, including Achilles tendinopathy, plantar fasciitis, metatarsalgia, sesamoiditis, tibialis posterior tendinopathy, medial tibial periostitis, and stress fractures, patellofemoral pain, and ilio-tibial band friction syndrome.
Over pronation can be corrected by the use of orthoses placed in the individual’s shoe.
Orthoses can be either preformed or (preferably) custom-cast to suit the individual athlete.
Many asymptomatic athletes over pronate—there is little or no evidence for the use of orthoses to correct this as a preventative measure.
Supination
Supination also occurs at the subtalar joint and normally occurs towards the end of the midstance phase of the gait to allow the foot to form a rigid lever in preparation for toe off.
The supinated foot is plantar flexed, inverted, and adducted.
Typically these individuals have a cavoid (high arched), rigid foot with poor shock absorption which predisposes to metatarsal stress fractures.
Excessive supination may also contribute to the development of ilio-tibial band friction syndrome.
Supination is much more difficult to correct with orthoses. Individuals should buy shoes with maximum shock absorption.
Footwear
Different sports require different footwear and individuals also have different footwear requirements.
Shoes consist of an upper (the part covering the foot) and sole (consisting of inner and mid-sole, wedge, and out-sole). Mid-sole is the main shock absorber and can be made of various materials with different inserts. Out-sole is designed for both traction and shock absorption, while the wedge increases heel height and aids shock absorption.
Upper should have a toe box providing adequate room and a firm heel counter to stabilize the subtalar joint and prevent excessive pronation.
The shape of the shoe can be straight or curved—a straight last shoe provides more stability.
Board lasting and slip lasting describes the way the upper of the shoe is attached to the sole. In board lasting the upper is attached to a hard inner sole board and is heavier and more stable.
Those with a tendency to over pronate require a running shoe providing more control—a straight (rather than curved) last construction, a combined last inner sole (i.e. board last to metatarsals, allowing more flexibility at the forefoot) with added medial support and a firm heel counter.
Tennis and other court shoes are generally constructed to provide more control and will be of a full board last construction.
Running shoes are not designed to allow sudden changes of direction and are unsuitable for sports involving a lot of twisting.
A high heel tab should generally be avoided as this may cause impingement on the Achilles tendon when the ankle is fully plantar flexed.
Shoes should be individual and sport-specific—those designed for distance running should provide stability and shock absorption, while those aimed at sports involving sudden changes in direction should provide good traction between the foot and the playing surface to avoid slipping.
Running shoes lose their shock absorbing qualities after about 500km, and should be changed frequently. Using worn-out footwear may lead to injury.
Football boots should allow the player to ‘feel’ the ball. Boots with ‘blade’ type cleats may increase the likelihood of some lower limb injuries, in addition to causing tibial lacerations.
Shoes designed for aerobic classes become worn after approximately 100h of activity.
Remember ask about the athletes leisure footwear as this may be a contributing factor as much as their sports footwear.
There is a recent movement towards barefoot running. The biomechanics of running are altered when wearing shoes and, in particular, the pattern of ground reaction force. This has led to a new generation of thin flexible running shoes. Although enthusiasts suggest this will reduce chronic over-use injury there is, as yet, little evidence.
Gait analysis
A detailed description of the techniques used in formal gait analysis is beyond the scope of this book. However, from the above discussion it is clear that the physician should have some understanding of the normal biomechanics of walking and running, and should be able to recognize abnormal gait patterns and refer appropriately for more detailed podiatric assessment.
Pronation is a normal component of the gait cycle and there is no evidence supporting the prescription of foot orthoses as a preventative measure in asymptomatic athletes who ‘over pronate’—these are generally individuals who have adapted and learnt to cope with their ‘abnormal’ gait and the introduction of orthoses into their shoes may cause considerable secondary problems.
Athletes should first be assessed standing from the front and then the posterior aspect.
Alignments such as persistent femoral anteversion will be obvious, producing a ‘squinting patellae’ appearance.
A pelvic tilt may be due to a leg length discrepancy—this can be formally measured from the anterior superior iliac crest to the medial malleolus with the athlete supine.
From the posterior aspect, the shape of the longitudinal arch and the angle between the Achilles and the calcaneus can be assessed— athletes who over pronate will tend to have a flat footed appearance with valgus heel position, producing the ‘too many toes’ sign.
The athlete should be asked to perform a half squat with the heels flat—this will reproduce the position of the foot in the mid stance phase of running and will demonstrate any tendency to over pronate.
The athlete should be observed walking in bare feet and if possible treadmill running in normal training shoes.
The athlete who supinates excessively will typically have a rigid high arched foot with rear foot varus alignment.
Core stability should be assessed, for example, by asking the athlete to perform a one leg squat and observing the degree of pelvic tilt and twisting that occurs during this manoeuvre.
Any abnormal gait patterns identified in a symptomatic athlete should prompt referral to a podiatrist for more formal gait analysis.
Several different types of orthoses are available, with the most appropriate usually being made from a cast of the athlete’s foot taken in the ‘subtalar neutral’ position.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree




