Abstract
Background and objectives
Elderly patients unable to get up after a fall or to activate an alarm mechanism are particularly at risk of complications and need to be monitored with extreme care. The different risk factors have fostered the development of stand-alone devices facilitating early detection of falls. We aimed at assessing performance of the Vigi’Fall ® system, a cutting edge fall detector associating a “passive release” mechanism attached to the patient and including external sensors; in the event of a fall, the system automatically triggers an alarm, and it also incorporates embedded confirmation software. We have put it to the test under real-life conditions so as to evaluate not only its efficacy, but also and more particularly its acceptability and tolerability in elderly subjects.
Method
The study ran from March 2007 through December 2008 in a geriatric ward with 10 subjects over 75 years of age, all of whom presented with a risk of falling.
Results
For eight patients wearing an accelerometric sensor, eight “falling” events and 30 “alarm release” events were recorded. Sensitivity and specificity of the device came to 62.5 and 99.5% respectively. For the two patients wearing the complete device, no events were detected. Not a single adverse occurrence was noted. Local tolerance was excellent in all but one of the subjects.
Conclusion
Our results clearly show that the device may be worn by patients without discomfort over prolonged periods of time, and also demonstrate that the verification component will help to increase sensitivity in real-life conditions to a level comparable to the level attained in our laboratory studies.
Résumé
Contexte et objectifs
Les patients âgés qui, après une chute sont incapables de se lever ou d’activer un dispositif d’alerte sont particulièrement à risque de complications et doivent être surveillés avec prudence. Cela encourage le développement de dispositifs autonomes permettant la détection précoce des chutes. Nos objectifs étaient d’évaluer la performance du système Vigi’Fall ® , un détecteur de chute de nouvelle génération associant un dispositif porté par le patient et des capteurs externes. Ce système déclenche automatiquement une alerte en cas de chute et incorpore un logiciel de levée de doute. Nous l’avons testé en conditions réelles pour connaître son efficacité mais surtout son acceptabilité et sa tolérance chez les sujets âgés.
Méthode
L’étude s’est déroulée de mars 2007 à décembre 2008 dans un service de gériatrie et a inclus dix sujets de plus de 75 ans qui présentaient un risque de chute.
Résultats
Pour huit patients portant le détecteur accélérométrique, huit événements « chute » et 30 événements « signal d’alerte » ont été détectés. La sensibilité et la spécificité de ce dispositif étaient de 62,5 et 99,5 %, respectivement. Pour les deux patients porteur de l’ensemble du dispositif, aucun événement n’a été détecté. Aucun événement indésirable n’a été noté. La tolérance locale a été excellente pour tous les sujets sauf un.
Conclusion
Nos résultats soulignent que le dispositif peut être porté par les patients pour des périodes prolongées, sans gêne et que le système de levée de doute pourrait contribuer à augmenter la sensibilité à un niveau aussi bon, en conditions réelles que dans nos études en laboratoire.
1
English version
1.1
Introduction
Since falls do not always entail direct and obvious consequences, they tend to be overly trivialized by doctors as well as patients, and their occurrence is grossly underestimated. Falls represent a major public health problem; not only do they constitute the main cause of morbidity and mortality in the elderly, but they also represent a prime reason for their institutionalization . Along with degenerative dementia, falls represent a prime object of research in gerontology.
As one ages, it becomes more and more difficult to rise up from the floor without assistance after a fall. In a study by Gurley et al., the average age of fallers found on the ground, at times dead, was 73, and 51% of them were women . Inability to get up from the floor is not only a distressing experience, but also a dangerous event entailing numerous consequences . Indeed, as was indicated in a study carried out at the Cochin Hospital emergency ward , several indirect elements tend to prove that mortality subsequent to a fall has more to do with the effects on metabolism of prolonged immobilization on the floor than with immediate traumatic consequences alone. Six months after passing through the emergency ward following a fall, 15% of the population had died. A multivariate analysis of the factors leading to mortality, with all causes taken into consideration, underscored the key factorial role of the initial Independence in Daily Living (or Katz) score; each subtracted point heightens the risk of death by 20%. The intrinsic causes of falling, the gender (masculine) and the metabolic consequences should also be taken into account. In any event, these conclusions draw attention to a population particularly at risk, namely subjects having been able neither to get up nor to sound an alarm, and who need to be monitored as closely as possible.
The above information underscores the need to draw up early alert strategies for falls. Notwithstanding steady growth of research in the field, the registration of more than 50 new patents and numerous publications, no reliable detection system is currently on the market; many technological roadblocks have yet to be overcome. A variety of procedures have been proposed; they would be applicable during different falling sequences. Initial research dealt with detection of the shock on the floor, after all, it is upon impact that velocity is dramatically reversed. Attendant detection systems are based upon finding the exact location of the reversed acceleration (or sudden “gear change”), and the sensors put to work are accelerometers and piezoelectric shock sensors .
Several teams subsequently focused on the detection of modifications in the speed of vertical shift. This system they have studied is based on pinpointing the location of the rapid acceleration of vertical velocity that occurs during the fall. Video analysis of falling patients has shown that while vertical and horizontal speeds are dissimilar when movement is mastered, they become close to similar during a fall; their modifications consequently allow for characterization of the latter . The main shortcoming of these methods is that detection thresholds are difficult to determine on account of the high degree of inter-individual variability of controlled displacement speeds. If the thresholds are too low, they lead to detection of falls that have not occurred. If, on the other hand, the thresholds are too high, actual falls may remain undetected. Several teams have tried to obviate these sources of error through supervised or unsupervised activity programs .
In view of enhancing detection capacities, these systems have combined different techniques: tridimensional accelerometers, inclinometers, vibration sensors, detector of angular velocity during transitions between vertical and horizontal positions . Finally, other sets of devices have been developed, for instance a tridimensional accelerometer placed close to the ear and comparing the acceleration to the experimentally set threshold velocities and a video camera activated by detection algorithms .
Recent research has confirmed the hypothesis that three-dimensioned accelerators enable reduction of the number of false alerts. Data collected during fall simulation have led to the conclusion that placing the sensor on the patient’s thorax generally enhances the reliability of detection .
To date, several fall detection devices have been withdrawn from the market on account of their pronounced deficient specificity and sensitivity. As of now, the most widely used system remains the classical remote alarm, which requires the patient’s active participation; in the event of an emergency, a button must be pressed. This system is evidently irrelevant when the patient is unconscious or for some other reason unable to put the apparatus to work .
The Vigi’Fall ® device ( Figs. 1 and 2 ) is presented as a cutting edge mechanism associating a micro-sensor borne by the patient with external infrared sensors coupled with confirmation software likely to render fall detection markedly more reliable. Triggering of the alarm involves taking into account the person’s location in his environment through combined analysis of the changes in activity registered before and after triggering of the accelerometric sensor and of the data delivered by the peripheral infrared sensors. In the case of a fall in which the person is unable to get up or call for help, an alert signal is immediately transmitted to a remote call center. An emergency procedure is thereby triggered, and it may prompt the intervention of a relative, a neighbor or an emergency service.

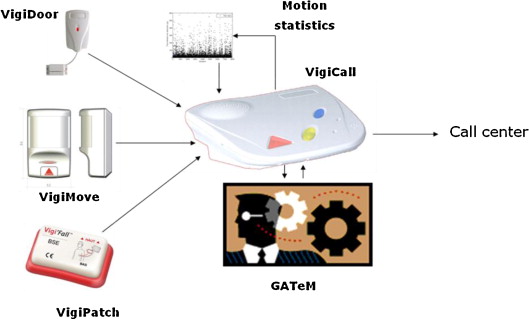
All in all, Vigi’Fall ® is able to distinguish the variations in movement connected with usual everyday activities from the unexpected movements involved in falls. One of the original features of the system consists in its taking into account not only the accelerometric signals, but also their being combined in terms of angular velocity.
1.2
Objectives
The main objective of our study was to evaluate under real-life utilization conditions the acceptability in elderly subjects of the cutting edge Vigi’Fall ® device.
Secondary objectives consisted in confirming the results obtained in laboratories with volunteers having carried out fall scenarios and in evaluating the relative specificity of the system’s overall performance.
1.3
Method
The study ran from March 2007 through December 2008 in the geriatrics ward of Broca hospital (AP–HP, Paris). Inclusion criteria for subjects in the study were the following: (i) subjects aged more than 75 years, (ii) presenting with a risk of fall assessed by the geriatrics doctor admitting the patient to the unit and (iii) having given their written consent to participate in the trial in accordance with the Declaration of Helsinki. The protocol had been approved by the institution’s ethics committee.
The patients initially benefited from a standardized clinical evaluation, after which they were required to permanently wear the accelerometric sensor of the Vigi’Fall ® device at the level of the thorax; it was held in place by an adhesive patch. They were made to lie down in rooms equipped throughout the experimentation with infrared sensors.
When the system detected occurrence of a fall, a signal was transmitted to an alert box indicating the patient’s room number and permanently borne by a nurse. The nurses were requested to specify in a standardized notebook occurrence of the two events “fall” and “alarm signal” along with their interactions (alarm signal triggered with or without occurrence of a fall; a fall detected without the alert having been signaled). Direct consequences of the fall, other eventual adverse effects and tolerance with regard to the device were likewise recorded. We postulated that over the course of a day, each patient would be likely to generate 30 movements brusque enough to trigger the apparatus, which would mean presenting 30 unplanned “alarm signals” a day.
Sensitivity and specificity were calculated through use of the formulas: Sensitivity = TP/(TP + FN) × 100 and Specificity = TN (TN + FP) × 100, where TP: true positives (fall detected), FN: false negatives (fall not detected), FP: false positives (alarm signal without fall) and TN: true negatives (absence of fall without alarm signal). In the same way, positive predictive value (PPV) = (FP/FP + TN), and negative predictive value (NPV) = (FN/TP + FN).
The data were collected on an IT support with the help of Excel 2003 ® (Microsoft) software. The results were given in mean ± standard deviation. Conditions for application were respected, and the risk of Type I error was of 5%.
1.4
Results
Ten patients were included. Eight of them wore only the accelerometric sensor, and the other two wore the complete device (accelerometric sensor, peripheral infrared detection system; and activation of the confirmation system).
The population’s average age was 83.4 ± 7.5 years. Average duration of use of the Vigi’Fall ® sensor was 21.0 ± 19.0 days with a total of 168 days for the group of eight and 28 days for the group of two subjects.
For the group of eight subjects using the accelerometric detector alone, 33 events were detected, with a mean score of 4.1 ± 5.4 events per patient, which were distributed amongst eight “Falling” events and 30 “Alarm” events ( Table 1 ). On the basis of these data, we deduced the device’s levels of sensitivity and specificity, which were the following: sensitivity = 62.5% and specificity = 99.5%. PPV was 16.7%, and NPV was 99.9%.
| Group 1 ( n = 8) Group 1 ( n = 8) Doubt removal component deactivated | Group 2 ( n = 2) Group 2 ( n = 2) Doubt removal component active | |||
|---|---|---|---|---|
| Alarm release | Fall | No fall | Fall | No fall |
| No alarm | 5 | 25 | 0 | 0 |
| Released | 3 | 5 040 | 0 | 840 |
For the two patients using the complete device, not a single event was detected ( Table 1 ).
Only one patient reported itchy sensations after 24 h with the sensor, but no rash or blotch was observed. This patient was the only one to leave the study and have the sensor withdrawn. No other adverse event was recorded. In all the other subjects, local tolerance was excellent, and none of them put a premature end to participation in the study. Duration of sensor use was limited by the fact that the patients were discharged from the ward when their hospitalization came to an end. System acceptability was deemed excellent; none of the patients reported any functional impairment over the course of the study. No premature discharge on account of poor acceptability was noted.
1.5
Discussion
Our study, of which the conclusions are preliminary, has the advantage of yielding results derived from use of the fall detector under real-life as opposed to experimental conditions. Even though these conditions correspond to hospitalization rather than home-based situations, such conditions have only exceptionally been brought into being. More precisely, studies reporting the results with obtained through use of similar devices have been based, for the most part, on protocolary experimental conditions under which the subjects included are required to carry out predefined sequences of “normal activities” , sequences that pronouncedly differ from the actual conditions of normal life.
The results reported in our study also seem quite promising as regards patients’ tolerance of the device, which can be worn all the time in daily life and over prolonged periods, without any impairment.
Moreover, our results are agreement with those of preliminary laboratory tests. Experiments have been conducted with Vigi’Fall ® on 14 volunteers who carried out more than 1000 scenarios ranging from an actual fall (520) to stumbling maneuvers (520). The results were high for both sensitivity (90%) and specificity (94%). However, the degree of sensitivity recorded on our “real-life” study (62.5%) remains insufficient insofar as it fails to eliminate the risk of an overly high number of false negatives, that is to say an overly high number of falls that go undetected by the apparatus. That said, it should be noted that most of the studied population was lacking in activation of the confirmation or verification system, of which the purpose is to heighten sensitivity so as obtain results as satisfactory as the results obtained experimentally.
Few studies have efficiently assessed the sensitivity and reliability of fall detection devices for the elderly. Computer research in the “PubMed” database using the keywords “fall detection sensor” yielded no more than 40 references. Examination of the different summaries shows that: (1) the prototypes from which results have been obtained are, for the most part, accelerometric devices; (2) Trials have been carried out mainly under experimental conditions or in a laboratory, and not under real-life conditions; (3) Sensitivity and specificity levels are only rarely mentioned in the published results .
Among the rare prototypes for which the articles actually present results, one may cite the case of a device developed in Switzerland that gave the alarm in 96% of “probable fall” or “fall” situations with no false positives . One may also cite an accelerometer worn at the wrist that is said to have avoided the occurrence of 65% of “traumatizing falls” without false positives over the course of 2 days under real-life conditions of use . Finally, a video camera system activated on the basis of detection algorithms was tested on 21 healthy volunteers having simulated falls of which 77% were detected, but with 5% of false positives .
Fleming et al. recently suggested that difficulties in getting up after a fall are significantly associated with aging, which tends to heighten the risks of motor and cognitive damage or impairment. They found no predictive characteristic for prolonged lying (or sitting…) on the ground other than the presence of cognitive disturbances. If this is indeed the case, then use of a detection system that would be automatically triggered by a fall appears vitally important. As a matter of fact, apparatuses necessitating a patient’s ability to trigger the system show their limits when in the event of cognitive disturbances. Results of a preceding study show that only 30% of the persons possessing a remote alarm device were actually able to use it to give an alarm and be promptly assisted and cared for following a fall having occurred at home .
By contrast, performances of the Vigi’Fall ® system have been assessed not only experimentally, but also from a real-life standpoint. Its high degree of specificity offers confirmation of the device’s ability to avoid false alarms. Up until now, however, the system has yet to show, once again in a real-life situation, a sensitivity allowing it to automatically give the alarm upon occurrence of a fall.
As we have just observed, automatic fall detection systems for the elderly are at the heart of today’s gerontechnology research. One should nonetheless bear in mind that these novel technologies need to be harmonized with the subject’s environment, and that a detector cannot advantageously replace the visits of family, friends and neighbors. Moreover, any detection system must function with consistent excellence in order to inspire confidence in the certainty of rapid intervention after a fall, so that negatively, the subject does not limit displacements within a home setting and that positively, everyday comforts be retained. We consequently strongly believe that detection systems need to be chosen and accepted by the elderly patient along with kith and kin.
In spite of a limited number of subjects, this study has yielded encouraging preliminary results. In order to provide further confirmation, another study is being envisioned. It will involve real-life conditions and include a larger number of patients having fallen; the aim will be to obtain enhanced sensitivity and specificity through use of a complete device including an accelerometric sensor, infrared, and a verification or confirmation system.
Disclosure of interest
J.-E. Lundy and J. Poujaud have ties with the company Vigilo S.A.–France. The other authors present no conflict of interest.
2
Version française
2.1
Introduction
Parce qu’elles n’ont parfois pas de conséquence directe apparente, les chutes ont tendance à être trop banalisées par les médecins et les patients, elles sont ainsi largement sous-évaluées. Les chutes représentent un réel problème de santé publique car elles constituent non seulement le principal facteur de morbidité et de mortalité chez les personnes âgées mais également d’entrée en institution : les chutes du sujet âgé sont donc, avec les démences dégénératives, un des axes prioritaires de recherche en gérontologie.
En vieillissant, il est de plus en plus difficile à se relever seul du sol après une chute : l’âge moyen des personnes retrouvées au sol ou mortes, dans l’étude de Gurley et al., était de 73 ans, 51 % étant des femmes . Cette impossibilité de se relever du sol est une expérience angoissante mais également dangereuse car elle peut avoir de nombreuses conséquences . En effet, comme l’indique une étude réalisée dans le service des urgences de l’hôpital Cochin , plusieurs éléments indirects tendent à prouver que la mortalité après une chute est liée aux conséquences métaboliques d’un maintien prolongé au sol plutôt qu’aux seules conséquences traumatiques immédiates. À six mois après un passage aux urgences pour une chute, 15 % de cette population était décédée. Une analyse multivariée des facteurs influençant cette mortalité, toutes causes confondues, mettait en évidence, comme facteur influençant la mortalité : le score de Katz initial, chaque point de moins sur l’indice initial augmentant de 20 % le risque de décès, les causes de chute intrinsèques, le genre (masculin) et les conséquences métaboliques. Ces conclusions mettent en lumière une population particulièrement à risque, celle n’ayant pu ni se relever ni donner l’alerte, qu’il convient de surveiller avec le plus grand soin.
Ces informations incitent à élaborer des stratégies d’alerte précoce des chutes En effet, malgré l’importance croissante de la recherche dans ce domaine, de plus de 50 nouveaux brevets déposés et de nombreuses publications, il n’existe pas aujourd’hui de système de détection fiable sur le marché car de nombreuses impasses technologiques demeurent. Différents procédés ont été proposés, intervenant à différentes séquences de la chute. Les premières recherches portaient sur la détection du choc au sol puisque, lors de l’impact, la vitesse s’inverse brutalement. Ces systèmes de détection sont donc basés sur le repérage de cette inversion du sens de l’accélération et les capteurs utilisés sont des accéléromètres et des capteurs de choc .
Plusieurs équipes se sont par la suite intéressées à la détection des modifications des vitesses de déplacement vertical. Ce système est basé sur le repérage de l’accélération rapide de la vitesse verticale qui survient lors de la chute. Il a été montré par l’analyse vidéo de patients chutant que les vitesses verticale et horizontale étaient dissimilaires pendant les mouvements contrôlés mais devenaient quasi-similaires pendant la chute : les modifications de ces vitesses permettent donc de la caractériser . Le principal problème de ces méthodes de détection est que les seuils de détection sont difficiles à déterminer en raison d’une importante variabilité inter-individuelle des vitesses de déplacement contrôlé. Si ces seuils sont trop bas, ils conduisent à détecter des chutes alors qu’il n’y en a pas. Inversement, s’ils sont trop hauts, on risque de passer à coté de chutes non détectées. Plusieurs équipes ont tenté de remédier à ces causes d’erreur par un apprentissage supervisé ou non .
Pour améliorer les capacités de détection, des systèmes ont combiné différentes techniques : accéléromètres tridimensionnels, inclinomètres, capteur de vibrations, et détecteur de vitesse angulaire au cours des transitions entre les positions verticales et horizontales . Enfin, d’autres dispositifs ont été développés utilisant, par exemple, un accéléromètre tridimensionnel placé près de l’oreille et qui compare l’accélération aux vitesses seuils fixées expérimentalement , ou une caméra vidéo activée par des algorithmes de détection .
Des recherches récentes ont confirmé que des accéléromètres en trois dimensions permettaient de réduire le nombre de fausses alertes. Les données, recueillies au cours de simulation de chutes, ont conduit à la conclusion que la localisation du capteur sur le thorax du patient était généralement plus appropriée pour une plus grande fiabilité de détection .
À ce jour, plusieurs des dispositifs de détection de chute mis sur le marché ont dû être retirés du fait de trop mauvaises spécificité et sensibilité. Le système le plus répandu à ce jour reste donc la classique télé-alarme qui exige la participation active du patient, qui doit appuyer sur un bouton en cas d’urgence. Ce système n’est donc pas pertinent lorsque le patient est inconscient ou n’a pas les capacités pour se servir de l’appareil .
Le dispositif Vigi’Fall ® ( Fig. 3 et 4 ) se présente comme un dispositif de nouvelle génération associant un micro-capteur porté par le patient et des capteurs infrarouges externes couplés à un logiciel de levée de doute permettant d’améliorer la fiabilité de la détection des chutes. Le déclenchement de l’alerte repose sur la prise en compte de la situation de la personne dans son environnement par l’analyse conjointe des changements du niveau d’activité avant et après le déclenchement du capteur accélérométrique de chute et des informations délivrées par les capteurs périphériques infrarouges. Dans le cas d’une chute où la personne est dans l’incapacité de se relever ou d’appeler à l’aide, une alerte est immédiatement transmise à un centre d’appels à distance. Une procédure d’urgence est alors déclenchée, ce qui permet l’intervention d’un parent, d’un voisin ou des services d’urgence.

Related posts:
 Efficiency of flexible derotator in walking cerebral palsy children
Efficiency of flexible derotator in walking cerebral palsy children
 Factors influencing the awareness of diabetic foot risks
Factors influencing the awareness of diabetic foot risks
 Assessment of quality of life in stroke patients with hemiplegia
Assessment of quality of life in stroke patients with hemiplegia
 Submental sensitive transcutaneous electrical stimulation (SSTES) at home in neurogenic oropharyngeal dysphagia: A pilot study
Submental sensitive transcutaneous electrical stimulation (SSTES) at home in neurogenic oropharyngeal dysphagia: A pilot study
 Tolerance and effectiveness on pain control of Pamidronate ®intravenous infusions in children with neuromuscular disorders
Tolerance and effectiveness on pain control of Pamidronate ®intravenous infusions in children with neuromuscular disorders
 Fate of abstracts presented at the 2008 congress of the French Physical and Rehabilitation Medicine Society
Fate of abstracts presented at the 2008 congress of the French Physical and Rehabilitation Medicine Society
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


