Essentials of Diagnosis
- Asthma, eosinophilia, and systemic vasculitis are the hallmarks of eosinophilic granulomatosis with polyangiitis (EGPA; Churg-Strauss syndrome).
- Classic clinical features include the following:
- Allergic rhinitis and nasal polyposis.
- Reactive airway disease.
- Peripheral eosinophilia (10–60% of all circulating leukocytes).
- Fleeting pulmonary infiltrates and occasional alveolar hemorrhage.
- Vasculitic neuropathy.
- Congestive heart failure.
- Allergic rhinitis and nasal polyposis.
- Approximately 50% of patients with EGPA have antineutrophil cytoplasmic antibodies (ANCAs), usually with a specificity for myeloperoxidase (MPO).
General Considerations
In 1951, Churg and Strauss reported a series of 13 patients with “periarteritis nodosa” (see Chapter 35) who demonstrated severe asthma and an unusual constellation of other symptoms: “fever…hypereosinophilia, symptoms of cardiac failure, renal damage, and peripheral neuropathy, resulting from vascular embarrassment….” The investigators termed this new disease “allergic angiitis and allergic granulomatosis,” and specified three histologic criteria for the diagnosis: (1) the presence of necrotizing vasculitis, (2) tissue infiltration by eosinophils, and (3) extravascular granuloma.
In 1990, an American College of Rheumatology panel liberalized the criteria for the classification of this disease, dropping the requirements for histopathologically proven vasculitis and granuloma (Table 34–1). The Chapel Hill Consensus Conference on nomenclature of the vasculitides subsequently defined the Churg-Strauss syndrome as a disorder characterized by eosinophil-rich, granulomatous inflammation of the respiratory tract and necrotizing vasculitis of small- to medium-sized vessels, associated with asthma and eosinophilia. In 2012, the Revised Chapel Hill Consensus Conference Nomenclature of Vasculitides recommended the term “eosinophilic granulomatosis with polyangiitis (EGPA)” for this disease. The purpose for this recommendation was twofold: (1) to emphasize certain cardinal features of the condition, and (2) for consistency with the names preferred for two related disorders, granulomatosis with polyangiitis (formerly Wegener granulomatosis)(see Chapter 32) and microscopic polyangiitis (see Chapter 33).
| Criterion | Definition |
|---|---|
| Asthma | History of wheezing or diffuse high-pitched rales on expiration |
| Eosinophilia | Eosinophilia >10% on white blood cell differential count |
| Mononeuropathy or polyneuropathy | Development of mononeuropathy, multiple mononeuropathies, or polyneuropathy (ie, stocking/glove distribution) |
| Pulmonary infiltrates, nonfixed | Migratory or transitory pulmonary infiltrates on radiographs |
| Paranasal sinus abnormality | History of acute or chronic paranasal sinus pain or tenderness, or radiographic opacification of the paranasal sinuses |
| Extravascular eosinophils | Biopsy including artery, arteriole, or venule, showing accumulations of eosinophils in extravascular areas |
EGPA is a rare disease—significantly less common than the other forms of ANCA-associated vasculitis. The annual incidence of EGPA is approximately 2.4 cases per million individuals. The distribution of cases is roughly equal between men and women. In recent years, associations between the use of leukotriene antagonists and EGPA have been reported. Rather than causing the disease, however, it is more likely that these medications permit the tapering of glucocorticoids, thereby “unmasking” the vasculitic phase of EGPA.
Clinical Findings
After the diagnosis of EGPA has been made, three disease phases are often recognizable: the prodrome, eosinophilia/tissue infiltration, and vasculitis.
The prodrome phase is characterized by the presence of allergic disease (typically asthma or allergic rhinitis). This phase often lasts for several years.
During the eosinophilia/tissue infiltration phase, striking peripheral eosinophilia may occur. Tissue infiltration by eosinophils is observed in the heart, lung, gastrointestinal tract, and other tissues.
In the third phase, vasculitis, systemic necrotizing vasculitis affects a wide range of organs, ranging from the heart and lungs to the peripheral nerves and skin (Figure 34–1).
Figure 34–1.
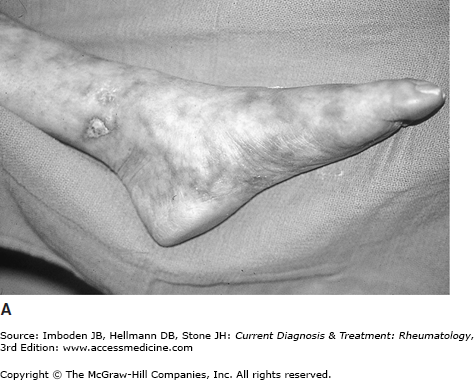
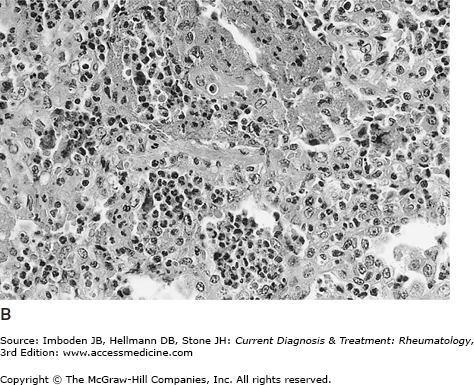
A: Foot of a patient with eosinophilic granulomatosis with polyangiitis (EGPA; formerly Churg-Strauss syndrome) showing livedo reticularis and a cutaneous ulcer just superior to the medial malleolus. The patient’s foot is held in extension because of a left foot drop (vasculitis neuropathy of the left peroneal nerve). B: Eosinophilic pneumonia in a patient with EGPA. Biopsy shows dense clusters of eosinophils within the lung parenchyma.
Upper airway disease in EGPA usually takes the form of nasal polyps or allergic rhinitis. A surprisingly high percentage of patients with EGPA have histories of nasal polypectomies, usually long before suspicion of an underlying disease is raised. Although pansinusitis occurs frequently, destructive upper airway disease is not characteristic of EGPA.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


