Elbow Fractures
David V. Lopez
Robert L. Kalb
The elbow consists of articulations of the distal humerus with the ulna and radius. The latter two articulate with each other to form the proximal radial ulnar joint. This chapter covers fractures of the distal humerus, the radial head, the olecranon, and the coronoid process and dislocations of the elbow.
FRACTURES OF THE DISTAL HUMERUS (SUPRACONDYLAR AND CONDYLAR FRACTURES)
Mechanism of Injury
A fall on an outstretched hand is common in the sporting and recreation settings, whereas a direct blow is more common in the occupational arena.
Diagnosis
There may be point tenderness pain, swelling, deformity, and instability of the elbow. As always, one should conduct a thorough neurovascular examination of the extremity.
Radiology
Anteroposterior, lateral, and oblique radiographs show the fracture. Computed tomography may be useful with condylar fractures. There is dissociation between the diaphysis and the humeral condyles with variable intercondylar extension (Fig. 1). Condylar fractures involve either the capitellum or the trochlea, or both.
Initial Treatment
The elbow should hang by the side and be immobilized with a posterior long-arm splint with the elbow flexed 90 degrees. A sling is used for support, and ice is used to decrease swelling.
Definitive Treatment
Fractures of the distal humerus require operative treatment if displaced. Refer displaced injuries for orthopedic evaluation.
When to Refer
Displaced fractures should be referred as well as any with neurovascular compromise.
Complications
Complications include stiffness, loss of motion, pain, malunion, and nonunion.
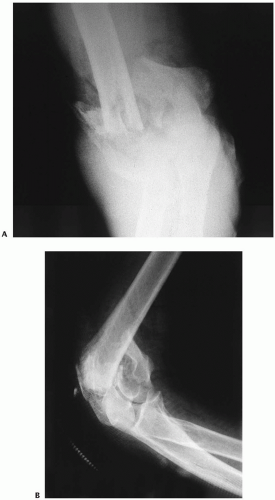 Figure 1 Anteroposterior (A) and lateral (B) x-rays that, due to bone overlap, poorly show the details of the fracture. (continues) |
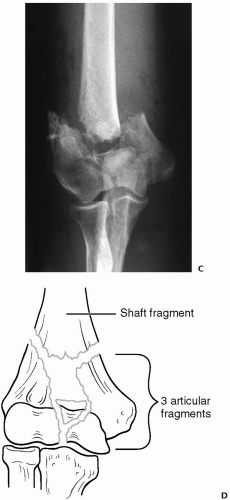 Figure 1 Continued. A traction x-ray (C) nicely shows the important details of the fracture and enables the surgeon to make a formal preoperative plan (D). |
FRACTURES OF THE RADIAL HEAD
Mechanism of Injury
Most commonly, fractures of the radial head result from a fall on an outstretched hand (Fig. 2).
Diagnosis
Tenderness localizes to the lateral side of the elbow.
Radiology
Radiographs should include anteroposterior, lateral, and oblique views. Forearm and wrist radiographs are done if tenderness is present. Fractures may be nondisplaced, displaced, comminuted (greater than two fragments), or associated with dislocation at the elbow or wrist.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


