Elbow Arthroplasty: History, Design Evolution, and Current Design Options for Treatment
Peter S. Johnston
Matthew L. Ramsey
HISTORICAL PERSPECTIVE
Normal elbow function requires a pain-free, mobile, and stable articulation.
Nonarthroplasty surgeries
Resection arthroplasty, interposition arthroplasty, and arthrodesis predominated prior to the advent of elbow arthroplasty.
ELBOW ARTHROPLASTY (HISTORY)
Development of total elbow arthroplasty (TEA) was borne out of the failures of nonreplacement surgeries to effectively treat articular and periarticular pathologies.
The elbow was felt to function as a rigid hinge.
Early efforts at elbow arthroplasty
Characterized by metallic, nylon, rubber, or acrylic hemiarthroplasties of the distal humerus or proximal ulna (FIG 1).
TEAs were metallic rigid hinged devices.
Predated the introduction of polymethylmethacrylate (PMMA)
Fixation of these implants to bone was achieved through uncemented intramedullary stems or extramedullary supports screwed into cortical bone (FIG 2).
Instability, early loosening, and unpredictable range of motion limited the success of these implants.
Poor implant fixation to bone and inferior implant design contributed to high failure rates from early loosening.
EVOLUTION OF ARTHROPLASTY (EARLY EFFORTS)
The modern era of total elbow replacement was initiated with the introduction of PMMA for implant fixation.9
The period of time following this achievement was characterized by a rapid evolution in the understanding of elbow biomechanics and surgical techniques and improvements in implant materials and design.
The failure of early efforts at arthroplasty led to two approaches to implant design.
Unlinked “resurfacing” designs
The joint is resurfaced with preservation of the collateral ligaments (FIG 3).
Success depends on the integrity of the soft tissue envelope, the presence of adequate bone stock to support the prosthesis, and the geometry of the articulation.
The contribution of the soft tissues to absorbing the forces across the elbow is believed to result in lower rates of implant loosening.
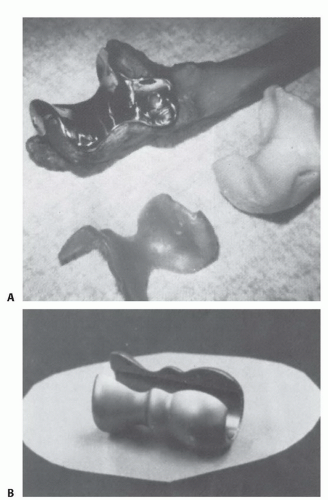
FIG 1 • A. Metallic resurfacing replacement of the proximal ulnar articular surface designed by Bickel and Peterson. B. Metallic distal humeral resurfacing replacement designed by Street and Stevens. Both implants were not stemmed and were poorly fixed to native bone. (A: From Peterson LFA, Jones JM. Surgery of the rheumatoid elbow. Orthop Clin North Am 1971;2:667; B: From Street DM, Stevens PA. A humeral replacement prosthesis for the elbow: results in ten elbows. J Bone Joint Surg Am 1974;56[6]:1147-1158.)

FIG 2 • A. Photograph of a linked, fully constrained hinged replacement. B. Clinical radiograph of the implant used to treat massive bone loss. Note the extramedullary fixation of the implant to native bone with cerclage metallic straps. (From Cooney WP, Morrey BF. Elbow arthroplasty: historical perspective and emerging concepts. In: Morrey BF, Sanchez-Sotelo J, eds. The Elbow and Its Disorders. Philadelphia: Saunders Elsevier, 2009:705-719.)
Linked “semiconstrained” designs
Stability is achieved through a coupled articulation between the humeral and ulnar components which allows a few degrees of varus-valgus and rotational laxity (FIG 4).
The ulnohumeral articulation tracks within the tolerance of the implant implying that the muscular envelope counters some of the forces across the elbow.29
EVOLUTION OF ARTHROPLASTY (MODERN EFFORTS)
TEA is in a period of refinement.
Clinical experience has demonstrated the design features that are acknowledged to contribute to success.
Anterior flange
Incorporated into many linked humeral designs
Felt to counteract posterior and rotational forces across the elbow contributing to implant loosening
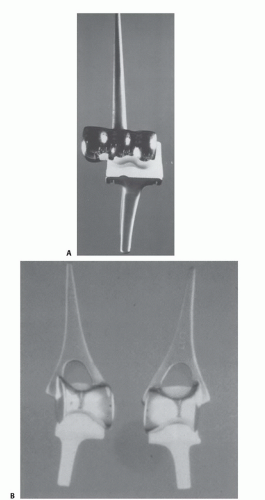
FIG 3 • A. The capitellocondylar resurfacing prosthesis. B. The Souter-Strathclyde resurfacing prosthesis. (From Cooney WP, Morrey BF. Elbow arthroplasty: historical perspective and emerging concepts. In: Morrey BF, Sanchez-Sotelo J, eds. The Elbow and Its Disorders. Philadelphia: Saunders Elsevier, 2009:705-719.)
Incorporation and hypertrophy of the bone graft behind the anterior flange proves that the graft becomes load bearing through stress transfer (FIG 5).
Stemmed implants
The addition of intramedullary stems to the humeral and ulnar components reduced the rates of component loosening.
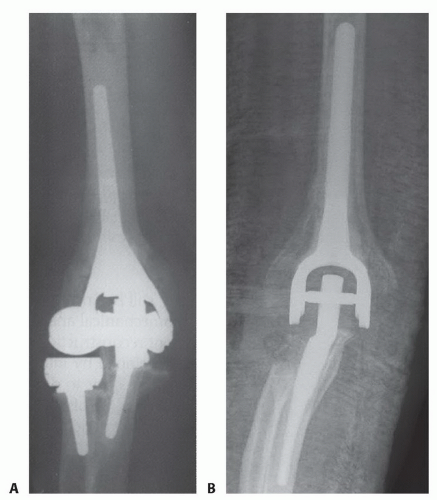
FIG 4 • A. The Latitude total elbow prosthesis. This is a hybrid implant that can be linked. Note that the implant allows for replacement of the radial head. B. The Nexel total elbow prosthesis is linked. There is no radial head component in this implant. (A: From Cooney WP, Morrey BF. Elbow arthroplasty: historical perspective and emerging concepts. In: Morrey BF, Sanchez-Sotelo J, eds. The Elbow and Its Disorders. Philadelphia: Saunders Elsevier, 2009:705-719; B: Reprinted with permission from Matthew L. Ramsey, MD.)
Cemented stems
Cement fixation of the implants is the current standard of care.
Cement technique is improved with brushing and lavage of the canals, use of PMMA in a more liquid state, and cement restrictors in the humerus and ulna to occlude the canal.12
EVOLVING ISSUES IN TOTAL ELBOW ARTHROPLASTY
Challenges remain with TEA that continue to fuel efforts to improve the outcome of surgery.
There have been numerous improvements in surgical techniques and implant design. These lessons can be broadly classified as implant fixation, instability, polyethylene wear and osteolysis (the articulation), and triceps dysfunction.
Implant fixation
The vast majority of implants are fixed to bone with PMMA.
Modern cement techniques have improved.12
Aseptic loosening has highlighted the need to continually explore alternative techniques of implant fixation.
Instability
Related posts:
 Arthroscopic Treatment of Posterior Shoulder Instability
Arthroscopic Treatment of Rotator Cuff Tears
Medial Clavicle Excision and Sternoclavicular Joint Reconstruction
Open Reduction and Internal Fixation of Nonarticular Scapular Fractures
Total Shoulder Arthroplasty for Glenohumeral Arthritis
Pectoralis Major Transfer for Long Thoracic Nerve Palsy
Arthroscopic Treatment of Posterior Shoulder Instability
Arthroscopic Treatment of Rotator Cuff Tears
Medial Clavicle Excision and Sternoclavicular Joint Reconstruction
Open Reduction and Internal Fixation of Nonarticular Scapular Fractures
Total Shoulder Arthroplasty for Glenohumeral Arthritis
Pectoralis Major Transfer for Long Thoracic Nerve Palsy

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


