Eden-Lange Procedure for Trapezius Palsy
Stephanie M. Gancarczyk
William N. Levine
DEFINITION
Trapezius palsy results from a disruption of cranial nerve (CN) XI, also known as the spinal accessory nerve.
Because the trapezius is innervated exclusively by CN XI, any disruption causes trapezius palsy.
The most common cause of trapezius palsy is iatrogenic.12
The trapezius plays an integral part in stabilization of the scapula, and dysfunction can lead to painful shoulder disability.
Nonoperative treatment, including strengthening of the functioning thoracoscapular muscles, does not typically provide satisfactory clinical results.2,5
Transfer of the levator scapulae, rhomboid major, and rhomboid minor (Eden-Lange procedure or triple transfer) is an accepted technique for this difficult problem.19
The procedure was first described by Eden6 in 1924 and then corroborated by Lange10 in 1951 and Francillon8 in 1955, all reporting satisfactory short-term results. Further modifications have improved on the initial procedure.1
Lateral transfer of the insertions of the three muscles allows the scapula to be stabilized in a position of abduction and anterior flexion.20
ANATOMY
The trapezius muscle is broad, superficial, and divided into superior, middle, and inferior fibers. Its origin is from the eternal occipital protuberance and medial third of the superior nuchal line, the ligamentum nuchae, and the C7-T12 spinous processes. It inserts on the acromion, clavicle, and spine of the scapula (FIG 1A).
The upper portion consists of descending fibers and functions as an aid to suspension of the shoulder girdle, allowing shrugging of the shoulder. The middle portion consists of transverse fibers and contributes to abduction and rotation of the inferior angle of the scapula. The ascending fibers of the lower portion (along with the serratus anterior) anchor the scapula to the chest wall.
Given its function to elevate and rotate the scapula, absence of the trapezius leads to drooping of the shoulder girdle and lateral winging of the scapula.
The blood supply is variable, but typically, the dorsal scapular and transverse cervical arteries supply the trapezius muscle.
In the posterior cervical triangle, CN XI is located in the subcutaneous tissue; this superficial location renders it susceptible to damage during procedures such as cervical lymph node biopsy.
Scapular winging occurs in both trapezius and serratus anterior palsy. In serratus palsy, the inferior angle of the scapula is noted to rotate medially (FIG 1B). This is the most common type of scapular winging. In trapezius palsy, the scapula rotates laterally (FIG 1C,D). Rarely, mild lateral scapular winging can occur in rhomboid palsy as a result of injury to the dorsal scapular nerve.18
PATHOGENESIS
The most common cause of CN XI palsy is iatrogenic. It is a rare but well-described complication of cervical lymph node biopsy and cervical mass excision.12,20,21
Other causes include trauma (including traction injuries) or injuries from other surgical procedures such as radical neck dissection.1
In one instance, a CN XI palsy was reported to have o ccurred after a viral infection.15
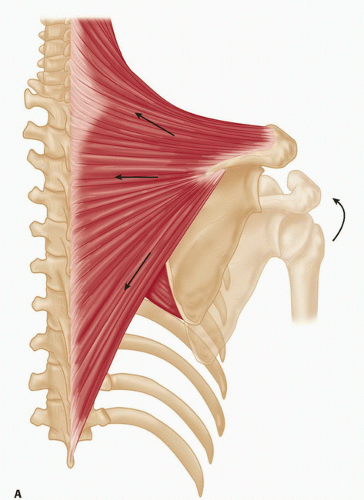
FIG 1 • A. Schematic of the three parts of the normal trapezius muscle: upper, middle, and lower. (continued)
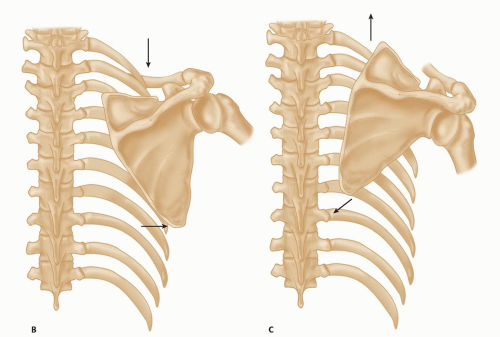
FIG 1 • (continued) B. Schematic of trapezius palsy, demonstrating lateral scapular winging and shoulder drooping. C. Schematic of serratus anterior palsy, demonstrating medial scapular winging.
Idiopathic CN XI paralysis also has been reported.7
Patterson13 reported trapezius palsy after acromioclavicular and sternoclavicular dissociation.
Even rarer causes include postcarotid endarterectomy and postcatheterization of the internal jugular vein.3
In most cases, patients report pain and present with visible deformity and dysfunction of the shoulder girdle.
NATURAL HISTORY
Trapezius palsy most often results from iatrogenic causes, as noted earlier, and, if left untreated, will lead to progressive worsening of the shoulder’s biomechanics and pain of the shoulder girdle.
Typically, the initial presentation is acute shoulder pain without palsy, with weakness of anterior elevation, and abduction appearing after a few days (with slow diminution of pain). Atrophy of the trapezius becomes clinically apparent after a few weeks.19
Radiating arm pain is thought to be the result of traction on the brachial plexus caused by drooping of the shoulder girdle.15
Although nonoperative management can provide reduction of pain, it does not lead to return of function, and patients treated without surgery usually go on to progressive shoulder dysfunction.
PATIENT HISTORY AND PHYSICAL FINDINGS
Altered mechanics of the entire shoulder girdle are possible with trapezius palsy.
The classic winging of the scapula seen in CN XI palsy is characterized by downward and lateral translation of the scapula.
The patient should be observed from behind so comparison can be made with the contralateral side.
Signs unique to CN XI palsy include lateral winging of the scapula (FIG 2A), an asymmetric neckline, wasting anteriorly due to involvement of the sternocleidomastoid muscle, drooping of the affected shoulder, pain, weakness of shoulder abduction, and forward elevation.16 Visible atrophy of the trapezius muscle should be noted19 (FIG 2B).
Symptoms include weakness made worse by prolonged use of the arm, a feeling of a heavy arm, and a dull pain radiating from the scapula to the forearm (and occasionally with radiation to the hand). The radiation of pain is described as mimicking thoracic outlet syndrome (medial aspect of the
upper limb). Pain typically is made worse by abduction of the shoulder as well as forward elevation.19 Some patients also reported paresthesias in the distribution of the auricular nerve (posterolateral side of the neck).19
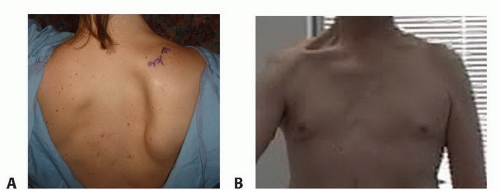
FIG 2 • A. Patient with a trapezius palsy demonstrating characteristic scapular winging. B. Anterior sternocleidomastoid muscle wasting due to the CN XI palsy.
Patients also often state that the arm feels difficult to control.15
Occasionally, patients are pain free and present only with winging and drooping of the scapula.
Range of motion is decreased in elevation as well as abduction and typically is limited to 90 degrees.15 Teboul et al19 report average active abduction of 78 degrees (range 30 to 140 degrees), and active forward flexion of 110 degrees (range 50 to 180 degrees). As a result, overhead activity is not typically possible nor is shrugging of the shoulder.
External rotation of the shoulder and elbow flexion are not affected by CN XI lesions.19
Reports of stiffness and passive range of motion are somewhat contradictory in the literature. Romero and Gerber15 state that patients did not always present with a stiff shoulder but passive range of motion typically was decreased. On the other hand, Teboul et al19 report that patients often presented with stiffness but with no deficit in passive range of motion.
Often, the diagnosis of CN XI dysfunction is one of exclusion, and it is not until an unsuccessful trial of physical therapy that a patient is referred for an electrodiagnostic study and CN XI palsy is confirmed.
The necessity for electrodiagnostic testing is an issue of debate in the literature. Romero and Gerber15 state that this testing is not necessary to establish the diagnosis of CN XI palsy but that it can be a valuable tool if other nerve lesions are suspected. Setter et al16 advocate electrodiagnostic testing as part of the initial workup.
Evaluate the scapula for signs of lateral translation by asking patient to perform a wall push-up.
CN XI palsy also affects the sternocleidomastoid muscle.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Related posts:
 Arthroscopic Treatment of Posterior Shoulder Instability
Arthroscopic Treatment of Rotator Cuff Tears
Medial Clavicle Excision and Sternoclavicular Joint Reconstruction
Open Reduction and Internal Fixation of Nonarticular Scapular Fractures
Total Shoulder Arthroplasty for Glenohumeral Arthritis
Pectoralis Major Transfer for Long Thoracic Nerve Palsy
Arthroscopic Treatment of Posterior Shoulder Instability
Arthroscopic Treatment of Rotator Cuff Tears
Medial Clavicle Excision and Sternoclavicular Joint Reconstruction
Open Reduction and Internal Fixation of Nonarticular Scapular Fractures
Total Shoulder Arthroplasty for Glenohumeral Arthritis
Pectoralis Major Transfer for Long Thoracic Nerve Palsy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


