Prolotherapy involves the injection of nonbiologic solutions, typically at soft tissue attachments and within joint spaces, to reduce pain and improve function in painful musculoskeletal conditions. A variety of solutions have been used; dextrose prolotherapy is the most rigorously studied and is the focus of this review. Although the mechanism of action is not clearly known, it is likely to be multifactorial. Data on effectiveness for temporomandibular dysfunction are promising but insufficient for recommendations. Research on the mechanism of action and clinical effects of dextrose prolotherapy are under way.
Key points
- •
Animal models suggest specific tissue responses to hypertonic dextrose, including proliferation.
- •
Clinical benefit in human studies is not explained by proliferation alone; the mechanism of dextrose prolotherapy (DPT) is likely multifactorial.
- •
DPT is efficacious for knee osteoarthritis and likely efficacious for finger osteoarthritis and Osgood-Schlatter disease.
- •
Moderate-quality randomized clinical trial (RCT) evidence supports use of DPT in rotator cuff tendinopathy, lateral epicondylosis, plantar fasciopathy and nonsurgical sacroiliac pain.
Introduction
Prolotherapy is an injection-based treatment of chronic musculoskeletal pain. A general surgeon in the United States, George Hackett, formalized injection protocols in the 1950s, based on 30 years of clinical experience. Prolotherapy has been identified as a regenerative injection therapy but is differentiated from other regenerative injection therapies, such as platelet-rich plasma (PRP) and stem cell injection by the absence of a biologic agent.
Prolotherapy is increasingly popular in the United States and internationally. The current number of practitioners of prolotherapy in the United States is estimated as several thousand based on conference attendance and physician listings on relevant Web sites, including both independent physicians and members of multispecialty groups. Currently, Prolotherapy Regenerative Medicine is one of the 23 specialty colleges of the American Osteopathic Association ( http://www.prolotherapycollege.org ). Training of doctors of medicine and doctors of osteopathy is primarily outside medical schools, for example, through postgraduate-level conferences and service learning projects through universities, professional organizations, and foundations ( www.fammed.wisc.edu/prolotherapy , www.aaomed.org , and www.hacketthemwallpatterson.org ).
Hypertonic dextrose is the most commonly used prolotherapy solution, with favorable outcomes shown in multiple clinical trials. It is inexpensive, readily available, and reported to be safe. This review focuses on the basic science and clinical evidence of prolotherapy using hypertonic dextrose solutions. The term dextrose is interchangeable with glucose because dextrose is the dexter (right-handed) form of glucose found in animals and humans. For this discussion, the term dextrose is preferred.
Introduction
Prolotherapy is an injection-based treatment of chronic musculoskeletal pain. A general surgeon in the United States, George Hackett, formalized injection protocols in the 1950s, based on 30 years of clinical experience. Prolotherapy has been identified as a regenerative injection therapy but is differentiated from other regenerative injection therapies, such as platelet-rich plasma (PRP) and stem cell injection by the absence of a biologic agent.
Prolotherapy is increasingly popular in the United States and internationally. The current number of practitioners of prolotherapy in the United States is estimated as several thousand based on conference attendance and physician listings on relevant Web sites, including both independent physicians and members of multispecialty groups. Currently, Prolotherapy Regenerative Medicine is one of the 23 specialty colleges of the American Osteopathic Association ( http://www.prolotherapycollege.org ). Training of doctors of medicine and doctors of osteopathy is primarily outside medical schools, for example, through postgraduate-level conferences and service learning projects through universities, professional organizations, and foundations ( www.fammed.wisc.edu/prolotherapy , www.aaomed.org , and www.hacketthemwallpatterson.org ).
Hypertonic dextrose is the most commonly used prolotherapy solution, with favorable outcomes shown in multiple clinical trials. It is inexpensive, readily available, and reported to be safe. This review focuses on the basic science and clinical evidence of prolotherapy using hypertonic dextrose solutions. The term dextrose is interchangeable with glucose because dextrose is the dexter (right-handed) form of glucose found in animals and humans. For this discussion, the term dextrose is preferred.
Methods
A search of electronic databases was performed by the University of Kansas library staff, including Medline, Web of Science, and ClinicalTrials.gov , from 1980 to 2016, without language restrictions. Search specifics included (1) prolotherapy; (2) (regenerative OR tendon OR tendinopathy OR ligament OR osteoarthritis) AND (dextrose OR glucose); and (3) dextrose injection from 1980 to 2016. Basic science studies were included in this review if they featured blinded histologic, histochemical, or radiographic outcome assessment. Clinical studies were included if randomized assignment was used and a dextrose arm was included. The strength of each RCT was assessed by 2 reviewers (K.D.R. and R.W.S.S.) using the Cochrane risk of bias tool. Disagreements were resolved by consensus and presented in descriptive and tabled form.
Results
Of 469 studies identified, 48 met inclusion criteria and were grouped into the following 2 areas: basic science (n = 33) and clinical research (n = 15).
Basic Science Findings
In vitro effects of dextrose on cytokine levels
Transport of dextrose into human cells uses a family of transport proteins, GLUTs 1–4, that interact with cytokines in a crucial way to signal either cell growth or repair. DNA expression changes favoring production of multiple cytokines have been measured within 20 minutes of exposure to in vitro elevation of pericellular dextrose levels to as little as 30 mM (0.54%) in a variety of animal and human cells, including fibroblasts, chondrocytes, and nerve cells.
Proliferative tissue changes in diabetic patients who have frequent elevations of pericellular dextrose in the 30-mM range are prominent, such as with diabetic proliferative retinopathy. Such effects are of unclear significance, however, given that elevated glucose levels in cases of diabetes seem to trigger interrelated complex pathophysiologic mechanisms, which may vary greatly from the effect of brief and isolated dextrose elevation on injection in either nondiabetics or diabetics. For example, the duration of glucose elevation is important to production of favorable or unfavorable cytokines.
Animal studies on cartilage and other soft tissue proliferation
Animal studies on femoral cartilage equivalent
Kim and colleagues reported chondrocytic tissue filling of 2-mm punch lesions in adult rabbit femoral cartilage on blinded histologic evaluation 6 weeks after injection of 10% dextrose or platelet-poor plasma but not in controls (noninjected). Histologic images were limited in this Korean language study. Park and colleagues demonstrated a protective effect of injector-blinded weekly 10% dextrose injection versus saline injection in a rabbit osteoarthritis model (anterior cruciate ligament [ACL] transection) on masked Mankin grading analysis at 19 weeks. The dextrose injection solution, however, contained amino acids and ascorbic acid as well, so the chondroprotective effect cannot be ascribed to dextrose alone.
Animal studies on Achilles tendon
A transient reduction in tensile strength of the healthy rat Achilles tendon was not demonstrable at 0 days, 5 days, or 10 days by Martins and colleagues after masked injection of 12.5% dextrose compared with normal saline injection or no injection. Injured rat Achilles tendon (transected and sutured) injected with 20% dextrose by Ahn and colleagues showed significantly more fibroblasts on blinded histologic review at 4 weeks compared with injured but noninjected control tendons. Kim and colleagues reported that single injection of either 5% dextrose (D5W) or 20% dextrose made hypertonic with saline (1100 mOsm) into noninjured rat Achilles tendon resulted in a significant increase in tendon diameter and fibroblast counts per high-power field (hpf) compared with equimolar (1100-mOsm) saline, suggesting a nonosmolar mechanism of dextrose-induced proliferation. In another study Kim and colleagues showed that oral nonsteroidal anti-inflammatory drug (NSAID) (celecoxib) administration did not limit the increase in Achilles diameter or fibroblast count per hpf at 6 weeks, suggesting a noninflammatory mechanism of proliferation.
Animal studies on medial collateral ligament equivalent
Jensen and colleagues demonstrated an inflammatory response to needling alone or needling with either saline or 15% dextrose in noninjured rat MCL. One measurable difference in the inflammatory responses was that, at 24 hours postdextrose injection, ED2 + macrophages and CD43 + leukocytes increased compared with saline-injection and needle-stick controls ( P <.05). Another study by Jensen and colleagues using MCL ligaments with a standardized subfailure stretch injury showed no significant differences in MCL strength or fibroblast number 3 weeks after injection with 15% dextrose or saline, although the cross-sectional area was significantly increased in the dextrose-injected MCLs ( P <.05). This time frame was short compared with other animal model studies, perhaps too short to evaluate the effect of dextrose.
Animal studies on transverse carpal ligament equivalent (subsynovial connective tissue)
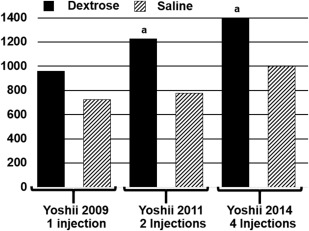
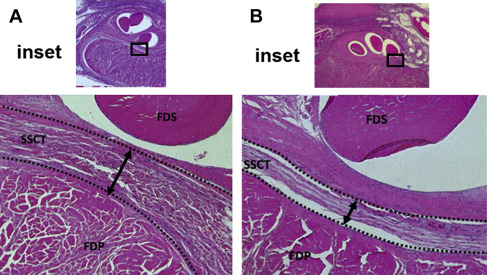
A study by Oh and colleagues demonstrated noninflammatory (no neutrophil invasion at 1 week, 2 weeks, 4 weeks, or 8 weeks) collagen bundle thickening at 8 weeks in the transverse carpal ligament rabbit equivalent after a single injection of 0.05 mL of 10% dextrose into the carpal tunnel equivalent (subsynovial space) through a small incision with a 30-gauge needle. This initial study was followed by 3 randomized, masked, 2-arm studies that compared 10% dextrose versus normal saline. One , two or four injections, given at weekly intervals, were evaluated in successive studies with findings measured at 12 weeks, 12 weeks, and 16 weeks, respectively, after the first dextrose injection. Energy absorption and load to failure of the subsynovial connective tissue (SSCT) were measured using a standardized approach. The 3 studies demonstrated consistent and significant increases in tensile load to rupture ( Fig. 1 ), total energy absorption to rupture ( Fig. 2 ), and thickening of the SSCT, presented in Fig. 3 graphically and by a representative biopsy in Fig. 4 .

Median nerve flattening was noted in the 2-weekly and 4-weekly injection studies along with a relative increase in latency of the median motor conduction ( P = .08), edema in the median nerve bundles, a thinner myelin sheath and observation of poorly myelinated nerve fibers, and evidence of wallerian degeneration. The author’s hypothesis that noninflammatory progressive transverse carpal ligament (or equivalent in animal) proliferative thickening (fibrosis) leads to eventual median neuropathy, is supported by these studies.
Human studies on cartilage and other soft tissue proliferation
Human studies on cartilage proliferation
Rabago and colleagues reported no changes in cartilage volume on blinded pretreatment and post-treatment MRI knee scans obtained at 1 year between dextrose-injected participants with symptomatic knee osteoarthritis and those who received saline injections or exercise prescription. Direct arthroscopic visualization of the joint surface, however, is superior to MRI evaluation, and a recent study by Topol and colleagues used pretreatment and post-treatment video-arthroscopy documentation, to compare pre and post treament denuded femoral cortex surfaces for evidence of cartilage growth. This was by methylene blue stain for chondrocyte growth, with biopsy of new areas of methylene blue uptake after treatment to evaluate for cartilage type (I = fibrocartilage and II = hyaline-like cartilage) by quantitative polarized light microscopy (QPLM) and immunohistologic straining with photographic documentaton of the biopsy defect area. Biopsies were obtained from areas of new uptake of methylene blue with photographic documentation of the biopsy defect area ( Fig. 5 ); QPLM and immunohistologic stains showed a mixture of fibrocartilage and hyaline-like cartilage in the biopsies. Although the study was limited by the small sample size of participants and the lack of a control group, it suggests that dextrose may stimulate or mediate chondrogenesis.
Human studies on ligament or tendon proliferation
Several studies have followed clinical and radiographic changes in parallel. Rabago and colleagues demonstrated clinical benefit from dextrose injection in lateral epicondylosis in the absence of demonstrable MRI changes at 16 weeks. Bertrand and colleagues used a systematic ultrasound rotator cuff tendinopathy grading method to evaluate pretreatment and post-treatment images and showed no significant differences at 9 months despite significant postprolotherapy clinical improvement. Two other second-look ultrasound studies have also indicated improvement in tendinosis, but these studies were not controlled, and standardization of ultrasound imaging is always challenging for clinical studies.
Human studies on a potential sensorineural mechanism
A direct sensorineural effect of dextrose injection has been proposed based on the observation that analgesia results from subcutaneous perineural injection of dextrose along tender peripheral nerves in some chronic pain patients. Hypothesizing a potential analgesic effect of D5W, Maniquis-Smigel and colleagues conducted a double-blind randomized controlled trial of the effect of epidural injection of D5W versus normal saline in 35 participants with chronic nonsurgical low back pain and buttock or leg pain. A significant analgesic effect was seen in those who received D5W in comparison to those who received normal saline from 15 minutes to 48 hours ( P <.05). The speed of analgesia onset after epidural or subcutaneous injection of dextrose suggests a potential direct effect of dextrose on peripheral nerves.
The transient receptor potential cation channel subfamily V member 1 (TRPV-1), formerly called the capsaicin receptor, is known to produce nociceptive pain with up-regulation. Bertrand and colleagues stimulated the TRPV-1 receptor using a capsaicin cream model to produce pain. Mannitol-containing cream or a control (vehicle) cream was then applied to the painful area in a double-blind manner. Mannitol is a 6-carbon sugar alcohol chemically related to dextrose. Pain resolution was reported faster with mannitol ( Fig. 6 ). Researchers hypothesized that the TRPV-1 receptors were down-regulated or that other related ion channels or receptors were directly affected.
Summary of basic science–related literature
Key findings from basic science studies are summarized in Box 1 . Basic science studies suggest that dextrose has independent effects that may promote local healing of chronically injured extra-articular and intra-articular tissue through stimulating both inflammatory and noninflammatory pathways; recent studies also suggest a direct sensorineural analgesic mechanism.
- 1.
Dextrose elevation to as little as 0.6% around fibroblasts and chondrocytes results in a rise in the level of complex proteins (cytokines) responsible to signal growth or breakdown of human tissue in vitro.
- 2.
The duration of dextrose elevation in vitro influences the balance of cytokines toward repair or disrepair.
- 3.
Dextrose injection (noninflammatory; 10%) may stimulate repair of rabbit femoral cartilage punch lesions.
- 4.
Dextrose injection (10%) may slow the development of osteoarthritis in a rabbit ACL-transection model.
- 5.
Healthy Achilles tendon in rats shows no temporary weakening after direct intratendinous injection.
- 6.
Healthy Achilles tendon in rats shows an increase in tendon diameter and an increase in fibroblast counts by DPT, which is not imitated by equimolar (hypertonic) saline injection and is not altered by administration of an NSAID, suggesting a mechanism of action not based primarily on hyperosmolarity or inflammation.
- 7.
Multiple randomized and saline injection–controlled injections under the transverse carpal ligament equivalent in rabbits demonstrate a consistent and significant thickening of the ligament and an increase in both tensile load to rupture and energy absorption to rupture.
- 8.
An increase in volume of cartilage in the human osteoarthritic knee has not been demonstrated after DPT.
- 9.
A chondrogenic effect of intraarticular dextrose in humans has been demonstrated in a small proof of concept study using second-look arthroscopy with cartilage cell staining and biopsy for immunohistologic evaluation of cartilage type showing a mixture of fibro and hyaline-like cartilage.
- 10.
Clinical studies on lateral epicondylosis with interval MRI testing and rotator cuff tendinopathy with internal ultrasonography have not shown a significant proliferation effect to explain clinical benefits, although evidence for improvement in tendinosis has been suggested in patellar tendinosis and plantar fasciopathy by interval ultrasound examination.
Clinical Research
The most important aspects of several studies that exemplify the effects of DPT in discrete conditions—osteoarthritis, tendinopathy, and low back pain—are summarized in this section.
Hand osteoarthritis
Trapeziometacarpal joint
Jahangiri and colleagues compared DPT to steroid injection in a 2-arm blinded trial ( Fig. 7 , Table 1 ). Participants in both groups with chronic thumb pain and trapeziometacarpal joint (TMCJ) osteoarthritis received 1-mL intra-articular and 1-mL extra-articular injection through the anatomic snuff box at 0 months, 1 month, and 2 months. Effects were assessed at 6 months by a 0 to 10 Visual Analog Scale (VAS) for pain, a Health Assessment Questionnaire Disability Index (HAQ-DI), and lateral pinch strength in pounds by a hydraulic pinch gauge.
| Source | Sequence Generation | Allocation Concealment | Blinding of Participants and Researchers | Blinding of Outcome Assessment | Incomplete Outcome Data Addressed | Selective Outcome Reporting |
|---|---|---|---|---|---|---|
| Jahangiri et al, 2014 | Low (A computer-generated randomization) | Low (sequentially numbered sealed envelopes used for assignment) | Unclear (information was not reported) | Unclear (clinician masked to group but who assessed outcome is not stated) | Low (5/60 lost to follow-up; <10%) | Low (clinical trial registration available) |
| Reeves & Hassanein, 2000 | Low (a random number table was utilized) | Unclear (clinicians and research coordinator masked. Assignments not made off-site | Low (the solutions were identical in color and viscosity) | Low (assessor and database coordinator were masked) | Low (lost to follow-up dextrose 2/13 and control 0/14; <10%) | Unclear (no protocol provided) |
Participants had statistically similar baseline characteristics. At 6 months the DPT group improved more in pain on movement (3.8 points ± 0.9 points [76%] vs 2.1 points ± 1.0 points [46%]; P = .02) and hand function (HAQ-DI) function score (3.0 points ± 2.2 points [65%] vs 1.77 points ± 1.0 points [41%]; P = .01) than the steroid group ( Fig. 8 ).
Trapeziometacarpal joint, proximal interphalangeal joint, or distal interphalangeal joint of fingers 2–4
Reeves and Hassanein compared DPT to blinded lidocaine injections in a 2-arm blinded trial ( Fig. 9 , see Table 1 ). Participants with chronic thumb or finger pain and radiographic hand osteoarthritis received treatment at 0 months, 2 months, and 4 months, with optional open-label dextrose injection after 6 months. All symptomatic joints were treated and participants were analyzed based on the average change across all joints treated, with effects assessed at 6 months (blinded) and 12 months (open label) using a 0 to 10 numeric rating scale (NRS) pain score and flexion range of motion.
Participants were similar statistically at baseline. The DPT group improved more in pain on movement (1.9 points ± 1.5 points [42%] vs 0.6 points ± 1.0 points [14%]; P = .027) and flexion range of motion (+8.0 ± 3.6° vs −8.8 ± 2.9°; P = <.01) than the lidocaine group at 6 months ( Figs. 10 and 11 ). DPT administration to the lidocaine group after 6 months resulted in a similar pattern of improvement as the original dextrose group.
Summary of hand osteoarthritis
Both HOA studies were double-blind trials but lacked a robust study design (see Table 1 ); whereas DPT is likely to be efficacious in HOA, higher-quality evidence is needed to confirm the role of DPT.
Intraarticular dextrose versus intraarticular lidocaine
Reeves and Hassanein compared DPT to blinded lidocaine injections in a 2-arm blinded trial using an intraarticular-only injection protocol ( Fig. 12 , Table 2 ) Participants with chronic knee pain and Kellgren-Lawrence (KL) stages II–IV radiographic knee osteoarthritis received injections at 0 months, 2 months, and 4 months, with optional open-label dextrose injection after 6 months. Primary measures were 0 to 10 NRS for walking pain and goniometrically measured knee range of motion.
| Source | Sequence Generation | Allocation Concealment | Blinding of Participants and Researchers | Blinding of Outcome Assessment | Incomplete Outcome Data Addressed | Selective Outcome Reporting |
|---|---|---|---|---|---|---|
| Reeves & Hassanein, 2000 | Low (a random number table was used) | Unclear (relevant information was not reported) | Low (identical control solution was used) | Low (assessor and database coordinator masked) | High (9/77 [11.7%]; >10%). | Unclear (no protocol provided) |
| Hashemi et al, 2015 | Unclear (randomization method was not mentioned) | Unclear (relevant information was not reported) | Unclear (relevant information was not reported) | Unclear (relevant information was not reported) | Unclear (relevant information was not reported) | Unclear (no protocol provided) |
| Dumais et al, 2012 | Unclear (random sequencing method not described) | Low (opaque sealed envelopes were used) | High (open-label trial) | Low (outcome assessors masked to group) | High (>10% lost to follow-up from each group) | Unclear (no protocol provided) |
| Rabago et al, 2013 | Low (random sequence generated by computer) | Low (off-site assignment and opaque sealed envelopes) | Low (both active and control solutions looked similar) | Low (outcome assessor masked to group allocation) | Low (no lost to follow-up cases) | Unclear (no protocol provided) |
Participants had statistically similar baseline characteristics. Range-of-motion gains favored the DPT group at 6 months (13.2 ± 2.1° vs 7.7 ± 2.2°; P = .015). The 2 groups did not have a statistically significant difference in walking pain ( Fig. 13 ).The DPT group, however, showed continuing improvement at 12 months and the lidocaine group, after unblinding, received DPT and also showed continuing improvement to 12 months (see Fig. 13 ).
Intraarticular dextrose versus intraarticular ozone
Hashemi and colleagues compared DPT to ozone injection in a 2-arm randomized open-label trial ( Fig. 14 ; see Table 2 ). Participants with KL I–II knee osteoarthritis of undocumented duration received 3 treatments at 7-day to 10-day intervals of intra-articular dextrose or intraarticular ozone. Effects were assessed at 3 months using 0 to 10 VAS pain levels and Western Ontario and McMaster Universities Arthritis Index (WOMAC), 0–100 points.
Participants had statistically similar baseline characteristics. At 3-month follow-up, the DPT group and the ozone group did not differ with respect to VAS pain level improvement (4.8 points vs 5.1 points) or WOMAC composite score improvement (25.3 vs 25.2) ( Fig. 15 ).This is a comparison, however, of 2 active treatment groups, both of which demonstrated significant improvement in pain and WOMAC scores compared with the pretreatment baseline.
Exercise plus intraarticular and collateral ligament dextrose injection versus exercise alone
Dumais and colleagues compared DPT plus a home-based physical therapy program to home-based physical therapy alone in a randomized crossover trial ( Fig. 16 ; see Table 2 ). Participants with chronic knee pain and any KL grading received injections at 0 weeks, 4 weeks, 8 weeks, and 12 weeks of 20% dextrose intra-articularly and 15% dextrose in collateral ligaments versus therapy only. Assessments were performed at week 16. After that, the 2 arms crossed over with a second assessment at week 36.
Participants had statistically similar baseline characteristics, and 86% were KL III or IV. Improvement in composite WOMAC score was significantly more in the group receiving DPT for period 1 (21.8 ± 12.5 vs 6.1 ± 13.9; P <.05) and period 2 (9.3 ± 11.4 vs 1.2 ± 10.7; P <.05) with an overall significance of P <.001 using a standard statistical method of crossover design analysis ( Fig. 17 ).







