Degenerative Joint Disease/Osteoarthritis
Jess H. Lonner
Eric B. Smith
 A 72-year-old man reports progressively worsening right knee pain. There is no history of trauma, though he used to play high school football. The knee feels stiff and swollen until he “gets it moving.” The pain has been waxing and waning over the last few years, with intervals of decreased pain followed by periods of more severe pain—now it is more painful on a daily basis, and it appears to be bowing. The pain is worse with activity and improves with rest. |
CLINICAL PRESENTATION
When evaluating an elderly patient with knee pain, it is important to remember that degenerative joint disease (DJD) is the most common cause of knee pain in such patients; additionally, the knee is the most common joint affected by osteoarthritis (OA).1
The clinical presentation of knee DJD is variable. The most common presentation will be an individual between the fifth to eighth decades of life with insidious knee pain, swelling, and stiffness that has gradually become more severe and more frequent. There is rarely a history of discrete trauma; however, occasionally patients may present after aggravating the knee with even a minimal twist or contusion. Patients may also describe a weather-related variation of their symptoms, with pain worse on cold, humid days. The pain is most often exacerbated by activity and relieved by rest. Patients will often relate a gradual decrease in their ambulatory tolerance. Patients with DJD can have night pain, especially after a day full of activity. However, unrelenting severe night pain should raise concern for diagnoses other than DJD, such as malignancy, gout, or infection.
Younger patients with previous knee trauma such as chronic anterior cruciate ligament rupture, tibial plateau fracture, osteochondritis dissecans, meniscus tear, femur fracture, or other injuries are at increased risk for knee DJD at an early age due to posttraumatic arthritis. It may also occur in the setting of chronic metabolic conditions (like gout) and obesity.
CLINICAL POINTS
OA or DJD is the most common cause of knee pain in older adults.
The knee is the most frequently affected joint by OA.
Pain may be worse in cold, humid weather.
Patients may report gradual decrease in ambulation tolerance.
PHYSICAL FINDINGS
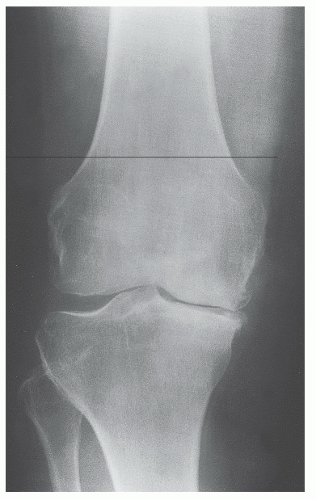
Physical exam findings of patients with suspected diagnosis of OA should begin with gross observation of gait. Patients with OA will often have an antalgic gait. Bowed legs (genu varum alignment) are most common in patients with OA. In such patients, the medial compartment is most affected by the degeneration. Alternatively, patients may present with a “knock-knee” deformity (genu valgum alignment) (Fig. 20-1). Such patients will often have more severe lateral compartment OA, with attenuation of medial structures in severe cases.
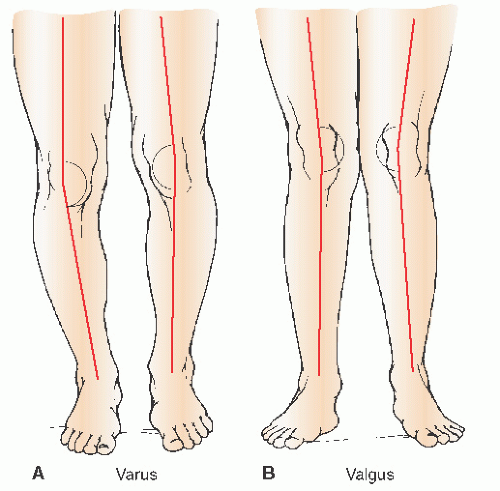 FIGURE 20-1. Varus and valgus alignment of the knee. A: In varus alignment of the knee, the angle formed by lines through the femur and tibia opens medially. B: In valgus alignment of the knee, the angle formed by lines through the femur and tibia opens laterally. (From Oatis CA. Kinesiology: The Mechanics and Pathomechanics of Human Movement. Baltimore, MD: Lippincott Williams & Wilkins; 2004.)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|




