Abstract
Aims
Our objective was to evaluate the specific effect of isokinetic muscle strength enhancement in the rehabilitation of obese subjects by comparing two groups (isokinetic muscle exercising associated with aerobic exercising or only aerobic exercising).
Patients and methods
This was a randomized, prospective study from January 2008 to December 2009 involving 40 obese patients randomized into two groups. The first group G1 ( n = 20) followed a program of aerobic training and isokinetic exercising of the extensor and flexor muscles of lower limbs and spine. The second group G2 ( n = 20) followed only a program of aerobic exercising. All patients completed their rehabilitation protocols comprising 3 sessions per week for two months. The parameters evaluated before and after the program were anthropometric parameters (weight, stature, body mass index, body fat and lean body mass percentages), cardiovascular parameters by stress test on electromagnetic ergo-cycle, an assessment of muscle strength by isokinetic dynamometer and an assessment of psychological status and quality of life.
Results
We recruited 36 women and 4 men. Initially, the 2 groups were comparable. After training, in both groups we noted an improvement in anthropometric parameters, with an average weight loss of 1.83 kg/week ( P < 0.001), an improvement in cardiovascular parameters with a decrease in heart rate at rest and under effort, and in systolic and diastolic arterial blood pressure values at rest and under effort ( P < 0.01 in both group), an improvement in parameters of muscle strength with increase in moment of maximum strength of extensor and flexor knee and spine muscles for all three test speeds, and an improvement in psychological status and in quality of life. The improvement of all these parameters was statistically greater in G1 ( P < 0.05).
Conclusion
Isokinetic muscle strengthening increases the effects of aerobic exercising in the obese by improving muscle strength, increasing lean body mass and reducing body fat.
1
Introduction
Obesity is today recognised as a major public health problem on account of its prevalence, the fact that it is developing fast in many countries in both adults and children, and the resulting overall cost for society.
Obesity is a multi-factorial, chronic problem; it constitutes a serious risk factor for several metabolic, cardiovascular and osteoarticular pathologies, and compromises psychological functioning and quality-of life among subjects concerned . It therefore follows that early, effective care is required on account of these various comorbidities .
Appropriate care for obesity should be multi-disciplinary, and based on a combination of therapeutic measures in the areas of diet, physical exercise, psychological support and, in some instances, bariatric surgery .
This care provision is necessary because, in addition to reducing overweight , it enables improvements on different parameters, such as cardiovascular risk factors , metabolic disorders , and functional and psychological repercussions, leading to improved quality of life . The treatment of obesity is constantly evolving. The use of an isokinetic dynamometer in the rehabilitation of obese subjects is a recent introduction.
The aim of the present work was to assess the specific effects of isokinetic muscle enhancement in the rehabilitation of obese subjects by comparing two groups, one undergoing isokinetic muscle enhancement in combination with aerobic exercising on a treadmill, and the other exercising solely on a treadmill.
2
Patients and methods
2.1
Patients
The study was prospective and randomised, and conducted in the physical medicine and functional rehabilitation department in Habib Bourguiba Hospital in Sfax (Tunisia) over a period extending from January 2008 to December 2009. The study was approved by the Tunisian research ethics committee.
2.1.1
Inclusion criteria
Obese subjects (BMI ≥ 30 kg/m 2 ), aged from 20 to 60 years and presenting a metabolic syndrome according to NCEP criteria . All the subjects signed written informed consent to participate in the study.
2.1.2
Exclusion criteria
We excluded all patients under 20 and over 60 years, those with a contraindication for effort tests , a contraindication for isokinetic evaluation , a serious psychiatric disorder or a disabling rheumatic pathology making the use of a treadmill impossible.
We recruited 62 patients, among whom 40 were retained for the study. The remaining 22 were excluded because they did not follow the rehabilitation protocol satisfactorily, either for health reasons or for reasons of distance from their homes.
The patients included were randomised into two groups:
- •
the first, G1, comprised 20 patients who followed a programme including both effort tests with exercises of a global type on a treadmill and isokinetic muscle enhancement sessions for the extensor and flexor muscles of the knees and spine;
- •
the second group, G2, comprised 20 patients who followed only a programme of effort tests with exercises of a global type on a treadmill.
2
Patients and methods
2.1
Patients
The study was prospective and randomised, and conducted in the physical medicine and functional rehabilitation department in Habib Bourguiba Hospital in Sfax (Tunisia) over a period extending from January 2008 to December 2009. The study was approved by the Tunisian research ethics committee.
2.1.1
Inclusion criteria
Obese subjects (BMI ≥ 30 kg/m 2 ), aged from 20 to 60 years and presenting a metabolic syndrome according to NCEP criteria . All the subjects signed written informed consent to participate in the study.
2.1.2
Exclusion criteria
We excluded all patients under 20 and over 60 years, those with a contraindication for effort tests , a contraindication for isokinetic evaluation , a serious psychiatric disorder or a disabling rheumatic pathology making the use of a treadmill impossible.
We recruited 62 patients, among whom 40 were retained for the study. The remaining 22 were excluded because they did not follow the rehabilitation protocol satisfactorily, either for health reasons or for reasons of distance from their homes.
The patients included were randomised into two groups:
- •
the first, G1, comprised 20 patients who followed a programme including both effort tests with exercises of a global type on a treadmill and isokinetic muscle enhancement sessions for the extensor and flexor muscles of the knees and spine;
- •
the second group, G2, comprised 20 patients who followed only a programme of effort tests with exercises of a global type on a treadmill.
3
Methods
3.1
Evaluation parameters
All the patients were assessed in two specialised consultations in the physical medicine and functional rehabilitation department and in the endocrinology department in the week preceding the start of the programme, and in the week following its termination.
3.1.1
Dietary survey
All patients were interviewed on their diet by the team of dieticians from the endocrinology department. These interviews enabled previous eating habits to be mapped out, and an assessment of weekly food intake. The data from these interviews were processed under BILNUT software, 1991 version, to translate it into energy intake in kilocalories, proportions of proteins, fats, carbohydrates and soluble sugars in grams/day, and in litres of fluid intake per day.
3.1.2
Evaluation of anthropometric parameters
The anthropometric parameters assessed were weight, stature, BMI and waist circumference (WC). For the assessment of lean mass and fat mass, and for basic metabolism, we performed a bioelectrical impedance measures with TANITA ® Model TBF-300.
3.1.3
Evaluation of cardiovascular parameters
These were assessed using the exercise stress test following the “modified Bruce” protocol , with a ZAN 680 Ergoline programme electromagnetic ergocycle. The parameters collected were heart rate at rest (HR r ) and under maximum effort (HR max ), systolic and diastolic blood pressure (SBP/DBP) resting (SBP rest /DBP rest ) and under maximum effort (SBP effort /DBP effort ), mean workload in watts, total duration of the effort in minutes and METS metabolic equivalents (calculated by the device).
3.1.4
Evaluation of muscular strength
Muscular strength parameters were measured by a Cybex ® Norm II Medimax isokinetic dynamometer, in terms of moment of maximum strength (MMS) or peak torque of flexor and extensor muscles of the knees (at the speeds 60°/s, 120°/s and 180°/s, and the flexor and extensor muscles of the spine at speeds 60°/s, 90°/s and 120°/s).
Following a warm-up of ten minutes on the ergometric cycles, the patient is positioned either seated to assess the knees, or standing for the spine. The range of the flexion–extension of the trunk was restricted to 70°. The protocol for isokinetic assessment consisted in three series of 5 repeats at each speed, for each knee, and for the spine. The three series were spaced by a recuperation period of one minute. The subjects were encouraged to do as best they could. Maximum isokinetic strength was defined as the mean value for the torque peaks at each repeat in Newtons × metre (Nm). All the tests were administered by the same investigator in the same conditions. The parameters collected for the isokinetic evaluation were the MMS or the torque peak for the flexors–extensors of each knee in Nm for each speed, and the mean power in watts for the flexors/extensors of both knees and the spine at the slowest speed 60°/s.
3.1.5
Evaluation of psychological impact
Anxious-depressive profile was assessed using the Human Anxiety and Depression Scale (HADS) . This scale comprises two columns, column A for anxiety and column D for depression. The maximum score for either of these columns is 21. A score between 8 and 10 indicates a possible anxious or depressive state, while a score over 10 confirms anxious or depressive state.
3.1.6
Evaluation of quality of life
Quality of life was assessed using the Arabic-language version of the Impact of Weight on Quality of Life-Lite scale (IWQOL-Lite) This scale comprises 5 domains: physical functioning, self-esteem, sexual life, social distress and work. The score for each item in these domains is reported as a percentage of the maximum possible score, giving a score ranging from 0 to 100. A score under 80% indicates that quality of life is impaired, and the lower the percentage the poorer the quality of life.
3.2
Rehabilitation protocol
3.2.1
Dietary prescriptions
For each patient, on the basis of the results of the dietary interview, a diet was prescribed, consisting in the following:
- •
a reduction of 25 to 30% in the previous calorie intake for patients whose spontaneous calorie intake was between 1500 and 3000 calories, and a reduction of 35% for those whose intake was above 3000 calories;
- •
a balanced distribution of different foods, with a mean percentage of 15% protein, 30–35% fats and 50–55% carbohydrates per ration;
- •
adequate fluid intake of 2 litres a day.
Compliance with the prescribed diet before and during the protocol was ascertained by a questionnaire at the end of the rehabilitation protocol. Compliance was considered “excellent” if the patient adhered to the diet throughout the protocol, “good” if the diet was correctly followed for at least 6 weeks, “moderate” if the diet was followed correctly for 3 to 6 weeks, and “poor” if the diet was followed correctly for under 3 weeks.
3.2.2
Exercising
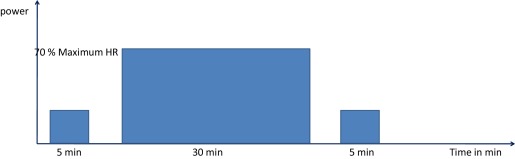
The exercising required was of a global nature, and performed on a treadmill. The intensity of the exercising was set at 70% of the HR max reached by the subject during the exercise stress test. As the protocol proceeds, with the improvement resulting from exercising, the target HR initially fixed at 70% of the HR max may no longer correspond to the same workload. The workload was thus increased as sessions progressed, retaining the same intensity at 70% of the HR max .
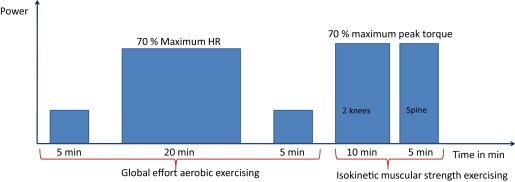
After initial warming-up on the treadmill for 5 min with a low workload, the exercising proper lasted 20 min for G1 and 30 min for G2 per session, followed by 5 min recovery at a low workload ( Figs. 1 and 2 ). In the course of the exercising session, cardiovascular parameters were monitored every five minutes (blood pressure and heart rate). All the patients had 24 sessions at a frequency of 3 sessions per week.
3.2.3
Isokinetic muscle strengthening
In addition to the global exercising, the patients in G1, in the same sessions, underwent isokinetic muscle strengthening of both knees and the spine ( Fig. 2 ).
For the knees, concentric isokinetic muscle strengthening was applied to the extensor and flexor muscles (hamstring and quadriceps) at 70% of the MMS at speeds 60°/s, 120°/s and 180°/s (according to an inverse pyramid) for 10 min, 5 min for each limb. At the end of the session, each patient underwent stretching exercises of both lower limbs.
For the spine, in the same session patients in G1 also underwent isokinetic concentric muscle strengthening of the flexor and extensor muscles at speeds 60°/s, 90°/s and 120°/s (inverse pyramid) at an intensity of 70% of the MMS for 5 min.
4
Statistical analyses
The data was analysed on SPSS 19 software. The following tests were used in this study: the Chi 2 test, ANOVA or variance analysis, regressions, and tests for comparisons of means for matched samples and for independent samples.
The Chi 2 test is used to study relationships between binary variables. We considered that a difference was significant if P > 0.05. Next, one-factor ANOVA analyses enabled univariate analyses on a dependent quantitative variable via a single-criterion (independent) variable. This enables the equality of means to be tested. Linear regression was used to test for significance of relationships between quantitative metric variables. The t -test for matched samples was used to study the evolution of values for the different clinical parameters, the effort tests, and muscular strength before and after the rehabilitation protocol. Student’s test for independent samples and the Chi 2 test were used to assess differences between groups at the outset. Student’s test for independent samples was also used for the comparison of means in the two groups after the protocol was complete.
5
Results
5.1
Anthropometric characteristics and evaluation of the impact of obesity
In our study, the mean age of the patients was 41,57 ± 10.03 years, range 20 to 56 years. The population was 90% female (36 women and 4 men). Obesity had been evolving on average for 8.75 ± 5.25 years on average, range 3 to 18 years. Mean weight was 98.4 ± 12.15 kg, range 84 to 137 kg. Mean BMI was 37.45 ± 4.94 kg/m 2 , range 30.1 to 48.1 kg/m 2 . Mean body fat was 48.99%, lean mass was 39.35%, and mean basic metabolism was 1854.85 ± 265.76 Kcal/day. The patients presented hypertension for 40% (16 patients), diabetes (type 2) for 37.5% (15 cases) and dyslipidaemia for 27.5% (11 patients).
The two groups were comparable for the different epidemiological and anthropometric data ( Table 1 ), for the different cardiovascular factors ( Table 2 ) and the muscular strength parameters for flexor and extensor muscles of the knees and spine at the start of the protocol ( Table 3 ).
| G1 | G2 | P | |
|---|---|---|---|
| Age (years) | 41.6 (20–56) | 41.6 (21–55) | NS |
| Sex (male/female) | 2/18 | 2/18 | NS |
| Clinical and anthropometric parameters | |||
| Hypertension | 9 | 7 | NS |
| Diabetes (type2) | 8 | 7 | NS |
| Dyslipidemia | 5 | 6 | NS |
| Weight (kg) | 98.3 | 98.6 | NS |
| BMI (kg/m 2 ) | 37.9 | 37 | NS |
| WC (cm) | 112.9 | 112.2 | NS |
| (%) of body fat | 47.6 | 50.5 | NS |
| (%) of lean body mass | 40 | 38.7 | NS |
| Parameters | G1 | G2 | P |
|---|---|---|---|
| HR rest (beat/min) | 87.5 | 83.4 | NS |
| Maximal HR (beat/min) | 158.9 | 159 | NS |
| BP rest (mmHg) | 135.8/83 | 133.3/85.8 | NS |
| Maximal BP (mmHg) | 198.9/101 | 188/97 | NS |
| Power (Watt) | 101.2 | 114 | NS |
| METS | 4.9 | 5.2 | NS |
Related posts:
 An alternative treatment for contractures of the elderly institutionalized persons: Microinvasive percutaneous needle tenotomy of the finger flexors
An alternative treatment for contractures of the elderly institutionalized persons: Microinvasive percutaneous needle tenotomy of the finger flexors
 Effect of submental sensitive transcutaneous electrical stimulation on virtual lesions of the oropharyngeal cortex
Barriers to home-based exercise program adherence with chronic low back pain: Patient expectations regarding new technologies
Intermittent catheterization in neurologic patients: Update on genitourinary tract infection and urethral trauma
Effect of submental sensitive transcutaneous electrical stimulation on virtual lesions of the oropharyngeal cortex
Barriers to home-based exercise program adherence with chronic low back pain: Patient expectations regarding new technologies
Intermittent catheterization in neurologic patients: Update on genitourinary tract infection and urethral trauma
 Muscle strengthening for hemiparesis after stroke: A meta-analysis
Muscle strengthening for hemiparesis after stroke: A meta-analysis
 A comprehensive picture of 4-year outcome of severe brain injuries. Results from the PariS-TBI study
A comprehensive picture of 4-year outcome of severe brain injuries. Results from the PariS-TBI study
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


