Chronic Carpal Instability
General Information
Injuries to the intrinsic and extrinsic carpal ligaments may alter the normal mechanics of the wrist, resulting in pain, disability, and possibly degenerative changes.
Diagnostic Criteria
Establishing the diagnosis of chronic carpal instability may be difficult. Diagnosis is made by synthesis of evaluations from repeated examinations as well as supporting radiographic imaging data.
History
Patients with chronic carpal instability usually present with complaints of pain in the wrist. This may be constant or associated with heavier activities. Their complaints may have been present for weeks, months, or even years. Although some patients may recall a specific injury to their wrist, many are unable to recall any significant injury. Depending on the type of instability (scapholunate, lunotriquetral, midcarpal, etc.), the pain may be located on the radial or ulnar aspect of the wrist. Patients may report a clicking or popping in their wrist with certain activities.
Physical Examination
A detailed examination of the wrist should be performed. This should include objective documentation of range of motion. Pain in certain positions of wrist motion should be noted. Tenderness should be elicited over the first dorsal compartment, the snuffbox, the scapholunate interval, the lunotriquetral interval, the distal radioulnar joint (DRUJ), the triangular fibrocartilage complex (TFCC), the pisotriquetral joint, and the midcarpal joint. Evaluation for
instability should be performed with the scapholunate instability, lunotriquetral shuck, and midcarpal instability tests. Comparison with the normal opposite wrist should be made.
instability should be performed with the scapholunate instability, lunotriquetral shuck, and midcarpal instability tests. Comparison with the normal opposite wrist should be made.
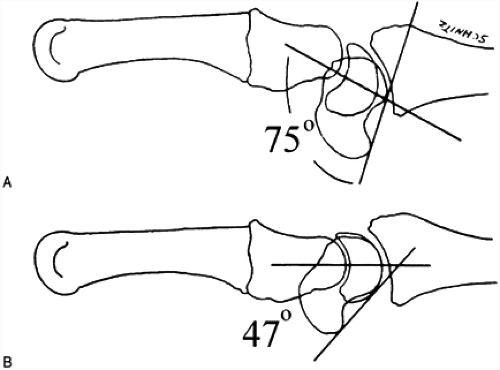 FIG. 1. A: Scapholunate instability is suggested by the increased scapholunate angle. Note the extended position of the lunate. B: The normal scapholunate angle is approximately 47 degrees. The lunate is oriented in a neutral tilt position (a line drawn from the peak of its convex surface through the valley of its concave surface is oriented parallel to the long axis of the radius).
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





