Casting and Splinting
The purpose of a cast or splint is to immobilize the extremity in a desirable position to allow healing of the injured structures and to prevent late stiffness. Knowledge of the anatomy of the injured structures dictates the position of immobilization. Although no one dressing is right for all injuries, some general principles do apply.
Hand dressings should be comfortable and durable. They should be applied firmly enough to prevent them from slipping, but not so firmly as to impede circulation or increase edema. The dressing should immobilize the parts that need to be immobilized and permit freedom of motion of uninjured parts.
Postoperative Dressings
Placement of a proper postoperative dressing is an essential part of any operative hand procedure. Inattention to detail may compromise the results of the surgery. A hand dressing is applied in a series of layers, each with its own purpose.
The wound is covered with a single layer of a nonadherent dressing (Xeroform, Adaptec) (Fig. 1). Petroleum-impregnated gauze is removed more easily from the wound than dry gauze. A single layer is used to allow blood and serum to seep from the wound.
Over the nonadherent layer, opened 4 × 4 or 4 × 8 are placed around the wound to provide a bulky support (Fig. 2). The gauze draws fluid from the wound into the dressing. The gauze is placed where immobilization is needed. Opened gauze is placed in the web spaces to prevent maceration of the digits if the fingers and wrist are to be immobilized. Too much gauze, placed tightly into the webs, can compromise the circulation of an injured finger. No immobilization of the fingers is required and no dressings are placed in the webs if only the wrist needs to be immobilized.
For dressings that include the wrist, the next layer consists of large gauze, foam, or polyester fiber pads that are applied to the dorsal and palmar surfaces (Fig. 3). The purpose of this layer is to provide padding and draw fluid away from the wound. These pads are placed to immobilize the hand in the desirable position. The wrist is splinted in 30 to 40 degrees of wrist extension (Fig. 4). This is accomplished
by aligning the long axis of the thumb with the long axis of the forearm. When the fingers also need to be immobilized in the dressing, the metaphalangeal (MP) joints are flexed 60 to 70 degrees and the interphalangeal (IP) joints are held in 10 to 15 degrees of flexion. The collateral ligaments of the MP joints are on stretch in flexion and the IP joints in extension. Failure to position the joints properly in the dressing may lead to a contracture. The thumb is positioned in abduction at the carpometacarpal (CMC) joint and extension at the MP and IP joints. The pads are held in place with circumferential roller gauze. Gentle pressure is used in applying the roller gauze to keep the pads snug to the wound, but not constrict the hand.
by aligning the long axis of the thumb with the long axis of the forearm. When the fingers also need to be immobilized in the dressing, the metaphalangeal (MP) joints are flexed 60 to 70 degrees and the interphalangeal (IP) joints are held in 10 to 15 degrees of flexion. The collateral ligaments of the MP joints are on stretch in flexion and the IP joints in extension. Failure to position the joints properly in the dressing may lead to a contracture. The thumb is positioned in abduction at the carpometacarpal (CMC) joint and extension at the MP and IP joints. The pads are held in place with circumferential roller gauze. Gentle pressure is used in applying the roller gauze to keep the pads snug to the wound, but not constrict the hand.
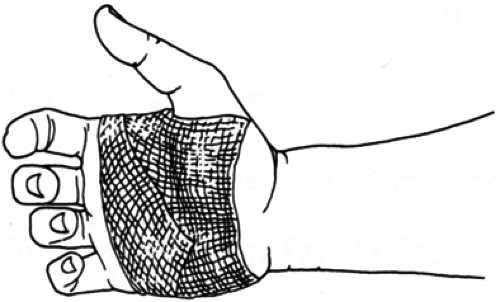 FIG. 1. Hand dressing: nonadherent gauze. |
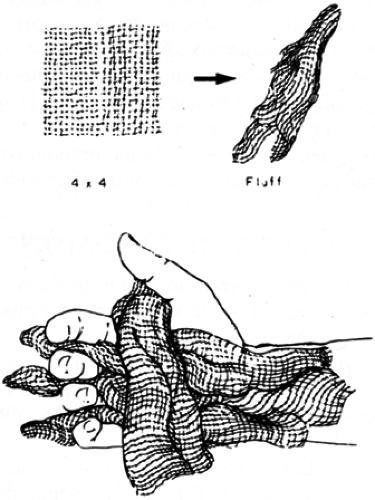 FIG. 2. Hand dressing: fluffy gauze. |
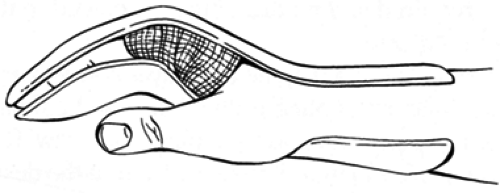 FIG. 3. Hand dressing: bulky adherent gauze. |
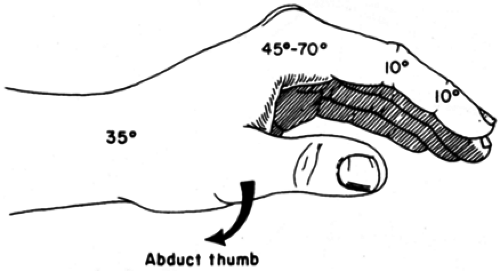 FIG. 4. Hand dressing: position of fingers. |
Finally, a plaster or fiberglass splint is applied to keep the soft dressing in the desirable position (Fig. 5). Splints are used rather than casts for postoperative dressings and after reduction of fractures and dislocations in order to avoid a circumferential hard layer that might lead to constriction with swelling. Plaster is used more commonly because it is cheaper and easier to mold. Ten layers of plaster are placed on the palmar surface to immobilize only the parts that require immobilization. A dorsal splint may augment a palmar one on occasion. Care should be taken that cast padding extends at least 1 cm past the splinting material to prevent contact between the skin and plaster. The plaster is held in place with a bias-cut stockinette or a loosely placed Ace bandage. The surgeon holds the hand in the desirable position while the plaster hardens.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


