Carpal Metacarpal Fractures and Dislocations
Thumb
Injuries to the carpometacarpal (CMC) region of the thumb include CMC dislocations, simple fracture dislocations (Bennett’s fracture), comminuted intraarticular fracture dislocations (Rolando’s fracture), and extraarticular fractures of the metacarpal base.
Diagnostic Criteria
Diagnosis is usually not difficult in the case of a Bennett’s, Rolando’s, or extraarticular fracture of the thumb metacarpal. Radiographic evaluation usually demonstrates conclusively the nature of these injuries.
History
These injuries usually result from a combination of axial loading and an abduction force to the thumb. This may occur during a fall or during a sporting event. A frequent mechanism of injury may be the impact of the thumb against the steering wheel or handlebar during a motor vehicle or cycling accident. If there is more of an axial loading component to the injury, this is more likely to result in a Rolando’s-type fracture.
Physical Examination
Evaluation of the thumb and hand generally reveals a substantial amount of swelling in the thenar region. The thumb may appear shortened and/or malrotated. Marked pain in this area may preclude further evaluation; however, crepitance may be noted. It may be possible to feel the CMC joint relocating
and resubluxing with manual pressure on the base of the thumb. Accurate diagnosis of the exact nature of the injury is not possible on physical examination alone.
and resubluxing with manual pressure on the base of the thumb. Accurate diagnosis of the exact nature of the injury is not possible on physical examination alone.
Radiographic Assessment
Anterior posterior (AP) lateral and oblique x-rays of the hand should be obtained. A true lateral of the carpometacarpal (CMC) joint should be obtained as well. A pure CMC dislocation usually represents a dorsal dislocation with disruption of the volar capsular ligaments. A Bennett’s fracture demonstrates an intraarticular fracture of the thumb metacarpal base with dorsal subluxation or dislocation of the thumb metacarpal. The size of the volar medial fragment is variable but because of the intact ligamentous structures to this piece, its relationship to the trapezium is usually normal (Fig. 1). A Rolando’s fracture is a comminuted fracture on the base of the thumb metacarpal. Typically, this may demonstrate a T- or Y-type pattern, but may be much more comminuted (Fig. 2). The degree of angulation of extraarticular fractures of the thumb metacarpal should be noted on the AP and lateral radiographic views.
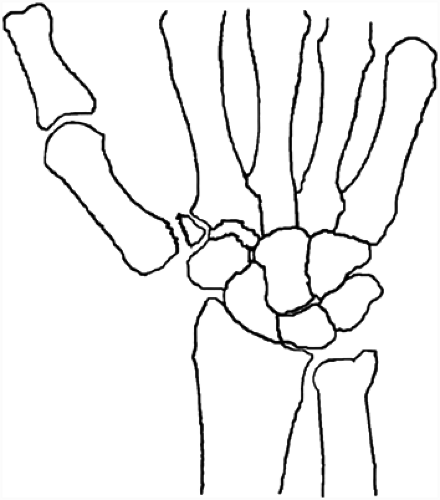 FIG. 1. A Bennett’s fracture results in subluxation of the major articular fragment (associates with the metacarpal), whereas the volar medial fragment maintains a normal relationship with the trapezium. |
 FIG. 2. A Rolando’s fracture represents a comminuted intraarticular fracture of the metacarpal base. A Y-type pattern is common. |
Treatment
Acute treatment of these injuries usually requires appropriate assessment of neurovascular status and temporary immobilization in a thumb spica splint. An attempted reduction should be performed if gross malalignment of the CMC joint is noted. In the case of a pure CMC dislocation, closed reduction is generally possible but significant instability may persist.
A stable CMC reduction and a basilar thumb metacarpal fracture with less than 30 to 40 degrees of angulation and no significant malrotation may both be treated to healing or union in a thumb spica cast. If any question regarding the stability or radiographic assessment of reduction of a CMC dislocation exists, then strong consideration should be given for operative management of this condition. Generally, closed reduction and percutaneous pinning under fluoroscopic guidance is possible. If a basilar metacarpal fracture is malrotated or requires reduction because of significant angulation, then percutaneous pinning or open reduction internal fixation (ORIF) is generally appropriate. Maintenance of a reduction of the thumb metacarpal is difficult with cast treatment alone because of the surrounding soft tissue of the thenar region.
Bennett’s and Rolando’s fractures require operative management. Frequently, a Bennett’s fracture may be managed with closed reduction and percutaneous pinning, especially when the minor fragment is small (Fig. 3). With a larger volar medial fragment, ORIF may be preferable to achieve a more
anatomic alignment of the articular surface. Treatment of Rolando’s fractures can be more challenging and usually requires ORIF and possibly bone grafting. External fixation and percutaneous pinning may be necessary in cases of severe comminution.
anatomic alignment of the articular surface. Treatment of Rolando’s fractures can be more challenging and usually requires ORIF and possibly bone grafting. External fixation and percutaneous pinning may be necessary in cases of severe comminution.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


