Biomechanics of the Glenohumeral Joint: Influence on Shoulder Arthroplasty
Luke S. Austin
Gerald R. Williams Jr.
Joseph P. Iannotti
INTRODUCTION
Pain relief and restoration of normal joint function are the goals of shoulder arthroplasty. To achieve this, the surgeon must restore flexibility to the capsular constraints, repair or rehabilitate the rotator cuff, deltoid, and periscapular muscles, and anatomically reconstruct the articular surfaces with an appropriately designed prosthetic implant. Normal glenohumeral joint anatomy is variable not only between individuals but also between the left and right side of the same individual. This variability makes prosthetic design and implantation complicated. However, understanding certain key and reliable anatomic correlations and biomechanical principles allows recreation of normal shoulder function not only a goal but also a reality in modern shoulder arthroplasty.
Extreme kinematic demands are placed on the shoulder joint. The normal shoulder is expected to position the arm in nearly all planes in space while providing a stable platform. The flexion extension arc of the shoulder can exceed 240 degrees with rotation as great as 180 degrees. To do this, the shoulder relies on a complex interaction between osseous and soft-tissue constraints. Osseous constraints in the shoulder are minimized to prevent impingement and soft-tissue constraints are maximized to ensure stability. This normal kinematic pattern requires a coordinated interplay between articular surface anatomy, capsular constraints, and rotator cuff, deltoid, and scapular muscle forces.
Several anatomic and biomechanical factors have been identified that may affect prosthetic design. Important anatomic factors include humeral head size and its orientation in three-dimensional (3D) space; humeral head shape; humeral head offset; humeral neck-shaft angle; glenoid size, shape, and orientation; glenoid offset; and lateral glenohumeral offset. Biomechanical factors that may influence prosthetic design and performance include glenohumeral articular conformity, glenohumeral articular constraint, periarticular muscular forces, and ligamentous restraints. Certain prosthetic characteristics, such as variability in humeral neck-shaft angle and version, humeral head offset, glenoid fixation and the shape of its interface with the native glenoid, glenoid metal backing, and material properties of the articulating surfaces, may influence prosthetic performance and clinical outcome. The purposes of this chapter are to review the current knowledge regarding relevant anatomic and biomechanical factors that potentially influence glenohumeral prosthetic design and to discuss the possible effects that variations in these design parameters may have on prosthetic performance.
ANATOMIC FACTORS
Humeral Head Geometry
Humeral head geometry is determined by humeral head size and shape. An in-depth understanding of humeral head
geometry is important in implant design. Small variations in humeral head geometry, especially thickness, can severely alter shoulder biomechanics.59,73,155
geometry is important in implant design. Small variations in humeral head geometry, especially thickness, can severely alter shoulder biomechanics.59,73,155
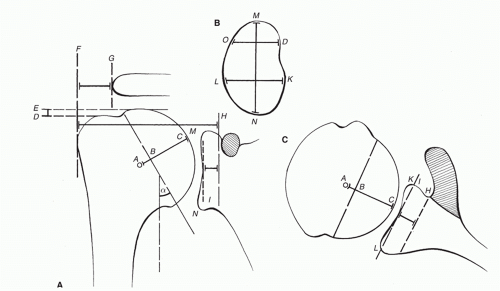 FIGURE 13-1. (A) Normal glenohumeral relationships depicted in the coronal plane include the humeral head center (A), humeral head radius of curvature (AC), humeral head thickness or neck length (BC), humeral neck-shaft angle (α), lateral glenohumeral offset (HF), greater tuberosity to acromion distance (FG), greater tuberosity to humeral head distance (DE), superior-inferior glenoid dimension (MN), and glenoid offset (HI). (B) The glenoid dimensions measured in the sagittal plane include the superior-inferior dimension (MN), the anterior-posterior dimension of the upper half (OD), and the anterior-posterior dimension of the lower half (KL). (C) The glenohumeral relationships in the axial plane include the humeral head center (A), the humeral head radius of curvature (AC), the humeral head thickness or neck length (BC), the anterior-posterior dimension of the glenoid (KL), and the glenoid offset (HI). (Reprinted with permission from lannotti JP, Gabriel JP, Schneck SL, et al. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am 1992;74:491.) |
Humeral Head Size
Humeral head size is strikingly variable between individuals. The articular segment is determined by the humeral head radius of curvature and humeral head thickness or neck length (Fig. 13-1). Mean humeral head radius is approximately 24 mm, with a range of 19 to 28 mm (Fig. 13-2), and are smaller for women than men.66,111 Mean humeral head thickness is approximately 19 mm, with a range of 15 to 24 mm (Fig. 13-3).66,111 Despite this variability some correlations can be made with relative consistency. First, both humeral head radius and thickness correlate with humeral shaft length and patient height.66,111 Next, the ratio of humeral head thickness to humeral head radius of curvature is remarkably constant at about 3:4 (0.7 to 0.9), regardless of patient height or humeral shaft size.66,111 Finally, the surface arc of the humerus available for contact with the glenoid is directly proportional to the ratio of humeral head thickness to humeral head radius and on average equates to a 150-degree arc of the humeral articular surface. This relationship is relatively constant, irrespective of humeral shaft length or patient height.68,109,111
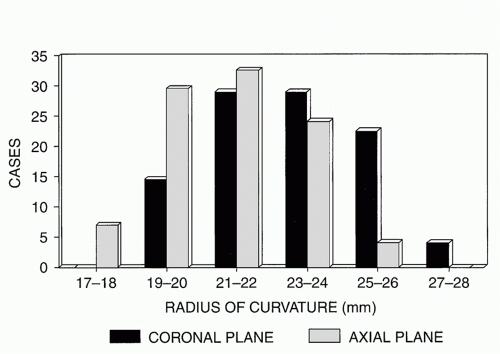 FIGURE 13-2. Humeral head radius of curvature fits a Gaussian distribution with a mean of 23 to 24 mm and a range of approximately 19 to 28 mm. Note that the axial plane radius is slightly smaller than the coronal plane radius. (Reprinted from Iannotti JP, Gabriel JP, Schneck SL, et al. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am 1992;74:491.) |
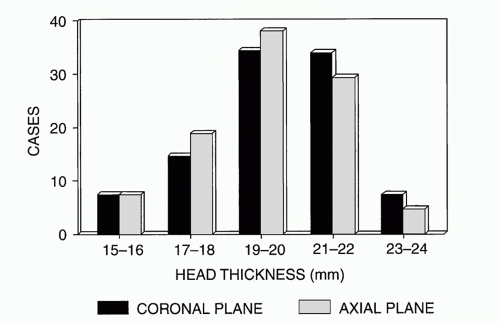 FIGURE 13-3. Humeral head thickness also demonstrates a bell-shaped distribution with a mean of 19 mm and a range of 15 to 24 mm. (Reprinted with permission from Iannotti JP, Gabriel JP, Schneck SL, et al. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am 1992;74:491.) |
Humeral Head Shape
The humeral head is not an entirely spherical structure. The shape of the humeral head varies not only in the coronal verse axial plane but also throughout the articular surface arc. The central 80% of the articular surface is spherical, with the coronal plane and axial plane radii of curvature being equal.1,24,66,88 However, in the peripheral 20% of the articular surface, the radius of curvature in the axial plane is, on average, 2 mm less than in the coronal plane (see Fig. 13-2). Therefore, the peripheral 20% of the humeral articular surface is elliptical, with the ratio of the axial plane radius to the coronal plane radius being 0.92.66 The clinical significance of this anatomic finding remains unclear. Theoretically, the elliptical shape of the humeral head may allow for increased obligate translation and improved range of motion. However, cadaver studies evaluating the range of motion and 3D kinematics of natural joints and joints reconstructed with spherical humeral heads show no difference.72 More recent cadaver studies of a direct comparison of a nonspherical prosthetic humeral head with the native humeral head and a spherical humeral head show a significant decrease in rotational range of motion and an increase in the translational motion of the humeral head with the spherical prosthetic humeral head, when compared to a nonspherical prosthetic or the native humeral head (Abstract ORS and AAOS 2012 San Francisco).60
Humeral Head Position
The position of the humeral head in relationship to the center of the humeral shaft and the transepicondylar axis must be thought of in three dimensions. A thorough understanding of this relationship is imperative in appropriate prosthetic implant positioning during shoulder arthroplasty, and malpositioning of as little as 4 mm can lead to increase subacromial impingement and decreased range of motion.155 The position of the humeral head can be accurately determined by describing the humeral head: (1) offset, (2) version, and (3) neck-shaft angle.
Humeral Head Offset
The center of the humeral head does not coincide with the projected center of the humeral shaft. Alternatively, the point in the proximal humeral metaphysis that corresponds to the center of the humeral head (assuming that the humeral head is a sphere) does not lie on a line projected proximally into the humeral metaphysis from the central axis of the intramedullary canal of the humeral diaphysis.7,13,93,111,121 The distance between the center of the humeral head and the central axis of the intramedullary canal is defined as the humeral head offset.7,13,111,121 Humeral head offset is commonly described in two planes, coronal and axial. Like most other proximal humeral anatomic parameters, reported humeral head offsets are variable.7,13,93,111,121 In the coronal plane, the humeral head offset is approximately 7 to 9 mm medial to the central axis of the intramedullary canal; in the axial plane, the humeral head offset is 2 to 4 mm posterior to the central axis of the intramedullary canal (Fig. 13-4).7,13,111,121 Humeral head offset is correlated with humeral head radius and humeral head thickness.111
Humeral Head Version
For a given humeral head radius, humeral head thickness, and humeral head offset in the coronal and axial planes, the location of the humeral articular surface may vary with respect to angle of rotation about the central intramedullary axis (i.e., humeral retroversion) and superior-inferior translation along the central intramedullary axis (i.e., head to greater tuberosity height). Humeral retroversion averages 20 to 30 degrees with a wide range of approximately 20 to 55 degrees.13,81,111,121 The vertical distance between the highest point of the humeral articular surface and the highest point of the greater tuberosity (i.e., head to greater tuberosity height) is approximately 8 mm and shows a relatively small range of interspecimen variability.66,111
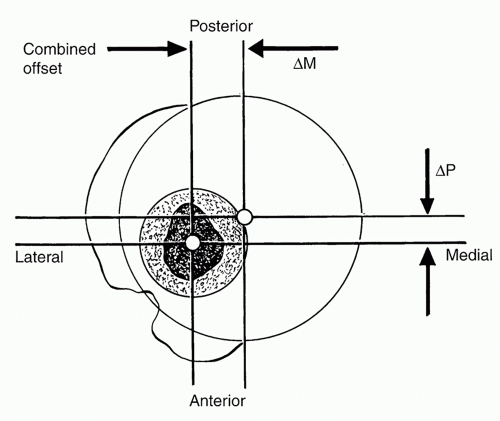 FIGURE 13-4. This axial plane section reveals the combined posterior and medial humeral head offset with respect to the central axis of the intramedullary canal. (Reprinted with permission from Boileau P, Walch G. The three-dimensional geometry of the proximal humerus. Implications for surgical technique and prosthetic design. J Bone Joint Surg Br 1997;79:857.) |
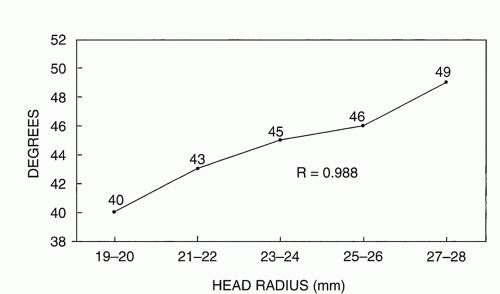 FIGURE 13-5 Humeral neck-shaft angle has been shown to correlate with humeral head size. (Reprinted with permission from Iannotti JP, Gabriel JP, Schneck SL, et al. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am 1992;74:491.) |
Humeral Neck-Shaft Angle
The neck-shaft angle is defined as the angle subtended by the central intramedullary axis of the humeral shaft and the base of the articular segment (see Fig. 13-1). The average neck-shaft angle is 40 to 45 degrees.13,66,93,111 However, more importantly, the humeral neck-shaft angle demonstrates significant individual variation with a range of 30 to 55 degrees.13,66,93,111 One study has shown a correlation between humeral head radius and neck-shaft angle, with larger humeral heads demonstrating larger neck-shaft angles (Fig. 13-5).66
Glenoid Anatomy
The glenoid is a complex structure that has been difficult to study until recently. The use of 3D computed tomography (CT) has allowed the anatomic parameters of the glenoid to become more accurately delineated. In describing glenoid morphology, multiple anatomic factors are considered, including (1) glenoid size and shape, (2) glenoid inclination and version, (3) glenoid offset and lateral glenohumeral offset, and (4) vault size and shape.
Glenoid Size and Shape
The size and shape of the articular surface of the glenoid can be defined by its linear superior-inferior and anterior-posterior dimensions as well as by its radius of curvature (see Fig. 13-1).66,93 The mean superior-inferior dimension of the glenoid (excluding the labrum) is approximately 39 mm (range 30 to 48 mm).66 The anterior-posterior dimension of the superior half of the glenoid is shorter than the inferior half of the glenoid, resulting in a pear-shaped or comma-like appearance. The mean anterior-posterior dimension of the superior half of the glenoid (excluding the labrum) is approximately 23 mm (range 18 to 30 mm), and the mean anterior-posterior dimension of the inferior half of the glenoid (excluding the labrum) is approximately 29 mm (range 21 to 35 mm).66 The ratio of the superior-inferior dimension to the anterior-posterior dimension of the larger, inferior half of an average glenoid is 1:0.7.66 The humeral head radius correlates with the size of the glenoid in both the superior-inferior and anterior-posterior dimensions (Fig. 13-6).66
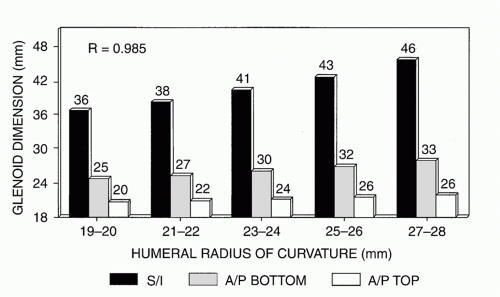 FIGURE 13-6 Humeral head size correlates with the superior-inferior dimension of the glenoid, the anterior-posterior dimension of the upper half of the glenoid, and the anterior-posterior dimension of the inferior half of the glenoid. A/P, anteroposterior; S/I, superoinferior. (Reprinted with permission from Iannotti JP, Gabriel JP, Schneck SL, et al. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am 1992;74:491.) |
Controversy exists with regard to the relationship between the glenoid and humeral articular radius of curvature.66,74,93,130 This controversy exists because of differences in measuring techniques, differences in sample sizes, and large individual variations in anatomy. The thickness of the articular cartilage of the glenoid increases toward the periphery of the articular surface and must be included when measuring the glenoid radius of curvature.130 However, even when the articular cartilage is included in the measurement, the radius of curvature of the glenoid articular surface does not equal the radius of the humeral articular surface in all specimens.66,74,93,130 Iannotti and colleagues66 observed that, on average, the glenoid radius of curvature in the coronal plane was 2.3 mm larger than the coronal plane humeral radius of curvature in the same specimen. Soslowsky and coworkers130 reported a difference between humerus and glenoid radii of curvature of less than 2 mm in 88% of specimens and less than 3 mm in all specimens. Kelkar and associates74,75 reported a mean humeral radius of curvature that was 2 mm less than the mean glenoid radius of curvature. In addition, as the humerus is abducted from a neutral position, the percentage of glenoid contact increases significantly, indicating that the functional conformity may increase during active elevation.148
Glenoid Inclination and Version
Glenoid inclination is defined as the angle between the superior-inferior axis of the glenoid surface and a line drawn from the middle of the glenoid to the junction of the scapular spine and the vertebral boarder of the scapula.22,46 The mean superior inclination of the glenoid is 4 degrees (range, 7 degrees inferior to 15.8 degrees superior) in males and 4.5 degrees (range, 1.5 degrees inferior to 15.3 degrees superior) in females.22 Obviously, the inclination angles between individuals are highly variable but the implications are not
entirely understood. However, Wong et al. published an association between increasing superior inclination and rotator cuff disease seen as superior migration of the humeral head.158
entirely understood. However, Wong et al. published an association between increasing superior inclination and rotator cuff disease seen as superior migration of the humeral head.158
Glenoid version is measured in a similar fashion, albeit, perpendicular to glenoid inclination with posterior angulations deemed retroversion. Multiple studies have assessed mean glenoid version and vary between 1.2 degrees (range, 9.5 degrees anteversion to 10.5 degrees retroversion)22 and 6 degrees (range, 2 degrees anteversion to 13 degrees retroversion).89 Glenoid version correlates with both race and gender. White patients demonstrate significantly more retroversion than black patients (mean 2.7 degrees compared to 0.2 degrees; p <0.00001) and males (mean, 1.5 degrees retroversion) trend toward more retroversion than females (mean, 0.9 degrees retroversion).22,89,137 Furthermore, glenoid version has been associated with multiple different shoulder pathologies, including osteoarthritis, rheumatoid arthritis, rotator cuff disease, and instability.34,35,46,124
Glenoid Offset and Lateral Glenohumeral Offset
The glenoid offset is defined as the perpendicular distance between the base of the coracoid process and the deepest portion of the glenoid articular surface (see Fig. 13-1). This distance determines the location of the glenohumeral joint line and is not correlated with humeral or patient size.66 The average glenoid offset is approximately 2 mm (range -5.0 to +5.0 mm).66
The lateral glenohumeral offset can be defined as the perpendicular distance from the base of the coracoid process to the most lateral extent of the greater tuberosity (Fig. 13-1).66 The distance from the most lateral extent of the greater tuberosity to the lateral edge of the acromion process correlates with the lateral glenohumeral offset and is easily measured intraoperatively (Fig. 13-1). The lateral glenohumeral offset is important in shoulder function because it determines capsular tension, resting length of the rotator cuff muscles, and the moment arm for the deltoid muscle. The lateral glenohumeral offset averages approximately 54 to 57 mm (range 43 to 68 mm), and the distance from the greater tuberosity to the lateral margin of the acromion process averages 17 mm (range 15 to 21 mm).66 Since the glenoid offset is less than 5 mm in all normal shoulders, it has little effect on the lateral glenohumeral offset.66 However, both lateral glenohumeral offset and greater tuberosity to acromion distance correlate with the humeral head size, which in turn correlates with the patient height (Fig. 13-7).66
Vault Size and Shape
Investigation into glenoid vault anatomy has been undertaken only recently. The use of CT scans with 3D reconstructions has allowed analysis of the complex geometry of the glenoid vault. Iannotti and colleagues evaluated 61 cadaveric scapulae utilized 3D CT scan reconstructions and developed a glenoid vault model. The glenoid was found to be regular in shape and roughly triangular in the superior-inferior dimension, which can be approximated by a model of stacked triangles.10 The glenoid vault shape is consistent among a wide patient population and is independent of glenoid size or patient gender (Fig. 13-8).10
 FIGURE 13-7. Lateral glenohumeral offset is defined as the distance from the base of the coracoid process to the lateral aspect of the greater tuberosity and is correlated with humeral head size. LHO, lateral humeral offset. (Reprinted with permission from Iannotti JP, Gabriel JP, Schneck SL, et al. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am 1992;74:491.) |
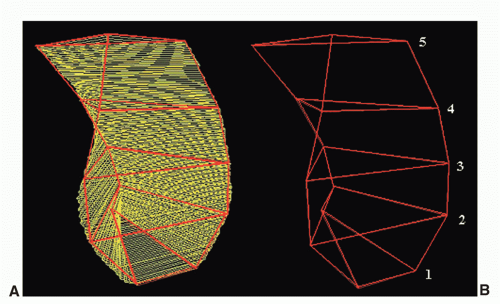 FIGURE 13-8. The shape of the glenoid vault can be approximated using a model of stacked triangles. (A) 3D CT scans of glenoid vault. (B) Model of stacking triangles representing glenoid vault geometry. (Reprinted with permission from Bennetts C, Gordiev K, Powell K, et al. Quantitative image analysis of glenoid vault shape. J Shoulder Elbow Surg, in review.) |
The consistency of the glenoid vault geometry has potential clinical applications. First, Iannotti and colleagues developed a set of five triangular implant prototypes designed to fit and fill the glenoid vault allowing for appropriate glenoid prosthetic component implantation in patients with articular surface compromise.25 Next, glenoid version in the pathologic shoulder is difficult to determine using standard radiographs and two-dimensional CT scans.15,20,103 The use of 3D CT scan imaging and a computer-generated glenoid vault model can more accurately determine native nonpathologic glenoid version and can help by assisting in preoperative planning for patients with posterior glenoid bone loss with osteoarthritis (Fig. 13-9).124
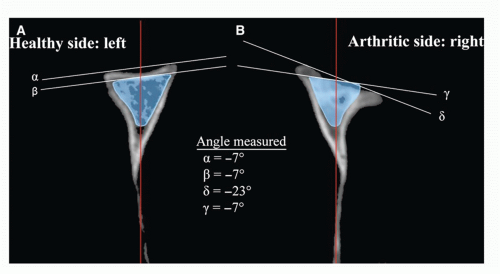 FIGURE 13-9. Example of glenoid version measurements after vault model placement in both scapulae of a subject with unilateral osteoarthritis. The plane of the scapula is represented by the red line. (A) On the healthy side, the glenoid version measures -7_ (α line), and the vault model also measures -7_ (β line). (B) On the arthritic side, the glenoid version measures -23_ (δ line). However, in the arthritic glenoid, the vault model measures -7_ (γ line), just as measured on the healthy, contralateral side. (From Scalise JJ, Codsi MJ, Bryan J, Iannotti JP. The three-dimensional glenoid vault model can estimate normal glenoid version in osteoarthritis. J Shoulder Elbow Surg 2008;17(3):487-491.) |
BIOMECHANICAL FACTORS
Glenohumeral Articular Conformity
Conformity of the articular surfaces refers to the difference between the radii of curvature of the humerus and glenoid. Congruent or conforming articulations are characterized by glenoid and humeral surfaces with equal radii of curvature. Incongruent or nonconforming articulations exist when the humerus and glenoid radii of curvature are not equal. In the normal shoulder, the components of the articulating surfaces include the humeral articular cartilage, glenoid articular cartilage, and glenoid labrum. The humeral articular cartilage is uniform in thickness throughout the entire articulating surface. As mentioned previously, the glenoid articular cartilage is thicker at the periphery than at the center.130 The glenoid labrum extends the arc of the articular cartilage and deepens the glenoid socket, but does not change the radius of curvature of the glenoid surface.63 The articular cartilage and glenoid labrum are reversibly deformable tissues. Therefore, for practical purposes, normal glenohumeral joints can be considered to be conforming if the humeral head radius of curvature is equal to or larger than the glenoid radius of curvature.71 Normal glenohumeral joints are considered to be nonconforming when the humeral head radius is less than the glenoid radius.71
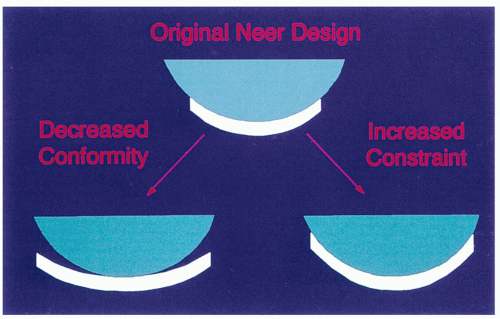 FIGURE 13-10. Conformity refers to the difference between the humeral head radius and the glenoid radius. Constraint is determined by glenoid wall height and is independent of conformity. Two articulations may have identical conformity and different constraints and vice versa. |
Conformity or congruence of the normal glenohumeral articulation is variable, as mentioned above in the section “Glenoid Size and Shape.”42,66,71,74,93 In the majority of specimens reported, the humeral head radius is within 2 to 3 mm of the glenoid radius.66,71,74,93 However, even small amounts of articular incongruence or nonconformity have important implications, with regard to glenohumeral kinematics during active motion.71
Glenohumeral Articular Constraint
Constraint is defined as the ability of the articular surfaces to resist translational motion of the humerus on the glenoid. The most extreme example of a constrained articulation is one in which the glenoid and humeral components are mechanically coupled to one another. In normal shoulders, where the glenoid and humerus are obviously not mechanically coupled, articular constraint is a function of the percentage of the humeral head covered by the glenoid. Articular constraint is correlated with glenoid wall height or, alternatively, socket depth, and is independent of articular conformity. In other words, different articulations may have equal conformities but different constraints, and vice versa (Fig. 13-10).
The normal glenoid is more constrained (i.e., has greater depth) in the superior-inferior direction than in the anterior-posterior direction.63,93 Additionally, the depth of the normal glenoid is contributed to equally by the articular cartilage and the glenoid labrum.63 In the superior-inferior and anterior-posterior dimensions, the glenoid articular cartilage and labrum combine to yield a socket that is 9 and 5 mm deep, respectively.63 Glenoid depth can also be thought of in terms of coverage of the humeral head.93 In the superior-inferior direction, the glenoid covers approximately a 65-degree arc of the humeral surface, compared to a 50-degree arc of coverage in the anterior-posterior direction.93
Periarticular Muscular Forces
The interactions between the many muscles that control motion of the shoulder girdle are extremely complex and beyond the scope of this chapter. However, in a simplified sense, the deltoid muscle provides power movement to the glenohumeral joint while the rotator cuff muscles compress the humeral head into the glenoid socket to provide a steering and stabilizing function.8,45,113,114 and 115,129,147 In a normal shoulder, the sheer force imparted by the deltoid and other large muscles is counterbalanced by the axial or compressive force imparted by the rotator cuff termed concavity compression.86 Concavity compression refers to the dynamic relationship between the force imparted to the humeral head on the glenoid by the rotator cuff and translation (i.e., stability) of the glenohumeral joint. This results in decreased humeral translation and increased joint stability certainly in the midranges of motion.87 The pathologic conditions that result in altered rotator cuff function, such as cuff tear arthropathy, may exhibit altered glenohumeral kinematics because of muscular imbalance between the rotator cuff and deltoid. In the worstcase scenario, the deficient rotator cuff may be unable to provide a sufficient enough fulcrum to allow elevation of the arm. Under these circumstances, anatomic prosthetic designs that depend on soft-tissue integrity for stability and function will not restore overhead function.
Ligamentous Restraints
The glenohumeral ligaments are thickenings of the joint capsule that are somewhat variable in their appearance.23,38,107,143,149 They act as checkreins to excessive rotation or translation of the humeral head at the extremes of glenohumeral motion.23,107,149 Although not entirely understood, the rotator cuff has attachments to the ligaments and may be able to tension these structures, therefore providing some stabilizing effects to the glenohumeral joint in the mid-range of shoulder motion. Various regions of the capsule act reciprocally to help stabilize the shoulder. The ability of the ligaments to control glenohumeral motion depends upon their location within the capsule as well as the arm position. The rotator interval capsule occupies the gap between the upper portion of the subscapularis and the anterior border of the supraspinatus. It consists of the superior glenohumeral ligament and coracohumeral ligament.31,58,150,151 The rotator interval capsule is primarily responsible for limiting external rotation and inferior subluxation of the humerus with the arm at the side.31,58,149,150 The middle glenohumeral ligament limits external rotation and anterior subluxation of the humerus with the arm in midabduction.107
The inferior glenohumeral ligament consists of an anterior band, an axillary pouch, and a posterior band.106,143 It is taut in abduction and therefore limits the degree of abduction as well as inferior translation of the humeral head in full abduction. The anterior band tightens in combined abduction and external rotation and therefore limits the amount of abduction and external rotation possible as well as anterior translation with the arm in this position.106,143,151 The posterior band is taut in abduction and internal rotation. Therefore, it limits the amount of simultaneous abduction and internal rotation possible and also limits posterior humeral translation with the arm in this position.106,143,151 The anterior and posterior bands can be made even more taut by passively positioning the abducted humerus posterior and anterior to the scapular plane, respectively.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


