 Applied Surgical Anatomy of the Approaches to the Ankle
Applied Surgical Anatomy of the Approaches to the AnkleOverview
The key structures that cross the ankle joint fall into specific groups.
Tendons
Three sets of tendons cross the ankle joint in addition to the Achilles and plantaris tendons, which lie posteriorly in the midline.
The flexor tendons—the tibialis posterior, flexor digitorum longus, and flexor hallucis longus (which are supplied by the tibial nerve)—pass behind the medial malleolus.
The extensor tendons—the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and peroneus tertius (which are supplied by the deep peroneal nerve)—pass in front of the ankle joint.
The evertor tendons—the peroneus longus and peroneus brevis (which are supplied by the superficial peroneal nerve)—pass behind the lateral malleolus.
The tendons are all prevented from bowstringing around the ankle by thickened areas in the deep fascia of the leg, called retinacula.
The different nerve supplies of the groups offer three potential internervous planes through which the ankle can be approached: medially, between flexors (tibialis posterior) and extensors (tibialis anterior); posterolaterally, between flexors (flexor hallucis longus) and evertors (peroneus brevis); and laterally, between extensors (peroneus tertius) and evertors (peroneus brevis).
Neurovascular Bundles
Two major neurovascular bundles cross the ankle joint and supply the foot. They present the major surgical concerns for all approaches around the ankle.
The anterior neurovascular bundle crosses the front of the ankle roughly halfway between the malleoli. It lies between the tibialis anterior and extensor hallucis longus muscles proximal to the joint (see Fig. 25-6) and between the tendons of the extensor hallucis longus and extensor digitorum longus muscles distal to the joint. The tendon of the extensor hallucis longus crosses the bundle in a lateral to medial direction at the level of the ankle joint (see Fig. 25-5).
The anterior tibial artery, which crosses the front of the ankle joint before becoming the dorsalis pedis artery, is palpable on the dorsum of the foot. It also communicates with the medial plantar artery through the first metatarsal space. Fractures through the base of the metatarsal bones and dislocations at the tarsometatarsal joint (Lisfranc’s fracture/dislocation*) can damage both elements of this anastomosis and cause ischemia to the medial side of the distal portion of the foot.
The deep peroneal nerve accompanies the anterior tibial artery. It supplies two small muscles on the dorsum of the foot: the extensor digitorum brevis and the extensor hallucis brevis. It also supplies a sensory branch to the first web space. Anesthesia in this web space is one of the first clinical signs of anterior compartment compression. Ischemia of the deep peroneal nerve occurs before ischemic muscle damage (see Figs. 25-5 and 25-6).
2. The posterior neurovascular bundle runs behind the medial malleolus, between the tendons of the flexor digitorum longus and flexor hallucis longus muscles (Figs. 25-1 and 25-2).
The posterior tibial artery passes behind the flexor digitorum longus before entering the sole of the foot, where it divides into medial and lateral plantar arteries (see Fig. 25-2).
The tibial nerve passes behind the medial malleolus with the posterior tibial artery. It gives off a calcaneal branch to the skin of the heel. After entering the sole of the foot, it divides into the medial and lateral plantar nerves, which supply motor power to the small muscles of the foot and sensation to the sole (see Fig. 25-2).
Superficial Sensory Nerves
Three major sensory nerves cross the ankle joint superficially, all supplying the dorsum of the foot. Knowledge of their course is vital in planning skin incisions. The sensory supply to the sole and heel comes from the lateral and medial plantar nerves, which are branches of the tibial nerve that lies deep at the level of the ankle.
The saphenous nerve is the terminal branch of the femoral nerve. It runs with the long saphenous vein in front of the medial malleolus, where it usually divides into two branches that lie on either side of the vein and bind closely to it. It supplies the medial, non–weight-bearing side of the middle part and the hind part of the foot (see Fig. 25-1).
The superficial peroneal nerve is a terminal branch of the common peroneal nerve. It crosses the ankle joint roughly along the anterior midline, where it usually divides into several branches. It supplies non–weight-bearing skin on the dorsum of the foot. The nerve is quite superficial at the level of the ankle joint; great care must be taken with skin incision in its area (Fig. 25-5; see Fig. 45-2).
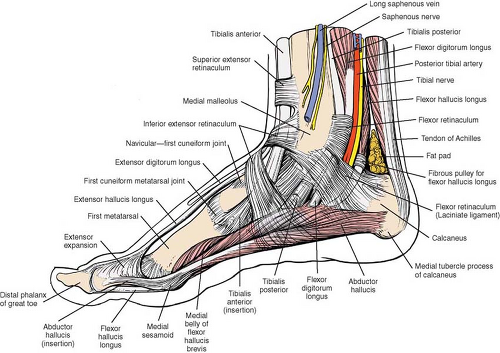
Figure 25-1 The superficial structures of the medial aspect of the foot and ankle. Fibers of the flexor retinaculum cross the neurovascular bundle, binding it to the medial side of the foot.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access
