Abstract
Avulsion fractures of the anterior superior iliac spine are rare. They usually occur in teenagers during sport activities. Cases concerning adults are very uncommon. We report here the case of a 23-year-old man who was admitted for recent pain of the left hip that worsened while kicking a ball in a soccer match eight days earlier. The examination found pain when moving the left hip in extension. Radiographs showed an avulsion fracture of the left anterior superior iliac spine, which was confirmed by computer tomography. The treatment was conservative consisting in rest and non-weight bearing with releasing of pain a few weeks later.
Résumé
Les fractures-avulsions de l’épine iliaque antérosupérieure sont rares. Elles surviennent le plus souvent chez des adolescents au cours d’activités sportives. Les formes chez l’adulte sont exceptionnelles. Nous rapportons un cas chez un jeune adulte de 23 ans. Il avait consulté pour une douleur inguinale gauche intermittente récente qui s’était exacerbée après un coup de pied dans un ballon lors d’un match de football huit jours auparavant. L’examen clinique retrouvait une douleur à la mobilisation de la hanche gauche en extension. La radiographie standard du bassin a montré une fracture-avulsion de l’épine iliaque antérosupérieure gauche, qui a été confirmée par une tomodensitométrie. Le patient a été traité orthopédiquement par du repos et mise en décharge du membre inférieur gauche, avec disparition de la douleur quelques semaines plus tard.
1
English version
1.1
Introduction
Avulsion fractures of pelvic apophyses are uncommon. They are often overlooked because confused with tendinitis or muscle tears. They occur in adolescents practicing sports. These fractures occur during growth from early apophyses ossification until their fusion with the corresponding pelvic tuberosities. They occur at the cartilaginous plate of the apophysis. During this period, apophyses where are inserted strong muscles, are the weakness zone of the musculoskeletal apparatus of young people. This weakness is reflected in the fragility of the enchondral ossification of the apophyses compared to biomechanical constraints exerted by the muscles. The lesions are usually due to a mechanism in tension at high sporting activities in subjects with an immature skeleton. Considering the number of teenagers practicing sport, apophyseal avulsions are rare. The most involved sports are football, athletics, skating and gymnastics.
Several cases of avulsion fractures of the anterior superior iliac spine (ASIS) were described in the literature, the majority involved children or teenagers practicing sport . Very rare cases have been reported in adults . We report a case of avulsion fracture of the ASIS in a young non-professional soccer player adult.
1.2
Observation
Mr RH is a 23-year-old young adult who presented for consultation with left groin pain. He had no particular medical history except unequal leg length unmatched. He complained for several weeks of intermittent left groin pain. The beginning was brutal during a shoot in the ball and did not result in functional impairment, the player continued the match. The patient had previously had, before the accident, some groin pain during hip flexion, but no grounds, because of their low intensity, to consult. Since the accident, the pain was mechanical in nature, absent at rest increasing in movement, without nocturnal awakenings. Given the persistence of pain, and after an exacerbation of pain after a soccer match played eight days ago, the patient consulted.
The clinical examination did not find on inspection any obvious deformity, ecchymosis or hematoma. On palpation, there was a sensitivity of the left ASIS and the area below. The flexion against resistance of the left hip was also sensitive. There was groin pain when moving the left hip in extension, free range of motion of the left hip and unequal leg length of 18 mm at the expense of the left limb. The neurological examination was normal.
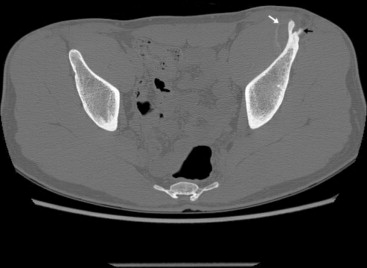
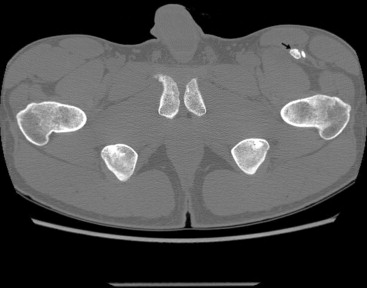
Plain radiographs of the pelvis found an avulsion of the left anterior superior iliac spine ( Fig. 1 ). The radiographic data were confirmed by a pelvic CT scan that showed an old avulsion of the left ASIS ( Figs. 2 and 3 ) with two fragments clearly at a distance. It showed also the avulsion of the sartorius and a calcic tonality condensing located to level of the left ASIS and going up along the internal cortical of the left iliac wing, evoking an old calcified hematoma ( Fig. 4 ). There was no contralateral injury.


The patient was treated by rest and partial non-weight bearing of the left leg with crutches during six weeks. There was no introduction of anticoagulant therapy or prescription of rehabilitation. The results were good with a disappearance of pain after a few weeks and a resumption of sporting activities after six weeks. There were no complications. Furthermore, compensation of leg length discrepancy was also recommended.
1.3
Discussion
Ossification of pelvic apophyseal nuclei occurs during adolescence. When the musculoskeletal chain of the adolescent is subject to large forces, the apophyses, which are the weakest link in this chain, will not resist. The muscles, tendons and ligaments are much stronger and more resistant than the areas of bone growth. These processes are found in different areas of the human skeleton like the tibial tuberosity and the lateral epicondyle of the elbow. In the pelvis, they are represented by the anterior iliac spines, the ischial tuberosity, the iliac crest and the pubic symphysis.
Among the apophyseal avulsions in the pelvis, avulsion of the ischial tuberosity is the most common, followed by avulsion of the ASIS, and that of the anterior inferior iliac spine . Some studies report a higher prevalence of fractures of the anterior inferior iliac spine compared to the anterior superior one . However, later closure of the apophyseal cartilage of the ASIS, between 20 and 25 years old, compared to the anterior inferior iliac spine (closure between 16 and 18 years old) argues for a greater frequency of fractures of the ASIS. Similarly, that explains their occurrence in older subjects and adults, as it is the case with our patient. The largest series of apophyseal avulsions of the pelvis has been described by Rossi and Dragoni. The series involved 203 avulsion fractures of the pelvis in 198 adolescent athletes. One hundred and nine interested the ischial tuberosity, 45 the anterior inferior iliac spine, 30 the ASIS, seven the pubic symphysis and three the iliac crest. Involved sports were soccer, basketball, gymnastics and athletics .
Avulsion fractures of the ASIS are rare. They are usually unilateral, but cases of bilateral and sequential fractures have been described .
Avulsion fractures of the anterior superior iliac spine occur most frequently in adolescents and young adults, mostly boys from 11 to 23 years old having sports activities (running sports, strike or jumping…) . The higher incidence among boys may reflect a greater tendency to practise sport or furthermore to practice high intensity sports in this class. These lesions can occur in any sport, but most involved ones are soccer, athletics, skating and gymnastics . The ASIS is more susceptible to fractures between 15 and 23 years old .
Fractures of the ASIS usually occur in the context of acute injuries, but chronic stress fractures, which can present as apophysitis, could be predisposing factors . The usual mechanism is often indirect by a sudden muscle contraction or a brutal stretch of an incompletely relaxed muscle attached to an immature bone during intense sports. It is rarely direct, secondary to direct trauma, or repetitive strain injury during training . Fractures of the ASIS can also occur when taking bone at the iliac crest for grafting . In our case, the avulsion of the ASIS was associated to unequal leg length. This combination appears to be fortuitous. To our knowledge, there are no data in the literature suggesting a relationship between cause and effect of unequal leg length and apophysitis or apophyseal avulsion.
Two muscles take their origin at the ASIS: the sartorius and the tensor fascia lata. They are bi-articular muscles. They cross over the hip and knee joints and they end at the tibia. In cases of fracture of the ASIS, one of these two muscles is dissected. It is more often the sartorius. The tensor fascia lata is rarely involved .
White et al. have described two types of fractures of the ASIS according to sport activity and according to the concerned muscle. They characterized the size of the fragment; the direction of its movement and the mechanism involved depending on concerned muscle . In ASIS fracture with avulsion of the sartorius, the injury occurs at racing in different sports, and the avulsed fragment is smaller and displaced anteriorly. In avulsion of the fascia lata, the mechanism is swinging a baseball bat, the avulsion occurring at the initial phase of batting. In these cases, the fragment was larger and displaced laterally .
Clinically, avulsion of the ASIS presents as a sudden and acute pain in relation to the ASIS occurring after a sudden movement. It is often associated with functional impairment in walking. Often, the patient reports an audible crack in the accident and evidence for growth apophysitis can also be found in history. The examination often finds pain on palpation of the ASIS. A thickening or hematoma can exist. Sometimes, the avulsed fragment of the ASIS is palpated under the skin . A meralgia paresthetica can exist; it is a complication of fracture by stretching or compression of the lateral femoral cutaneous nerve . A very suggestive sign is represented by the onset of pain to passive stretch of the concerned muscle and to its contraction during isometric testing. In the case of our patient, the old pain that was prior to the sports injury and the calcified hematoma would be in favour of an old injury, probably an apophysitis, which would have been aggravated by an avulsion fracture at the soccer game.
Plain radiographs of the pelvis, with sometimes three quarter radiographs, usually allow to confirm the diagnosis, by showing the fracture and the potential displacement . Sometimes, apophyseal injuries may be radiographically occult if the apophysis is not ossified or only minimally so. In this case, ultrasonography has the advantages of early detection even without ossification center. The sonographic examination shows a hypoechogenic zone in the region of the apophysis extending to the surrounding soft tissue, representing oedema or haemorrhage, widening of the normally hypoechoic physis between the apophysis and the pelvis, dislocation of the apophysis, and mobility of the apophysis on dynamic examination. Power Doppler sonography can also be used showing hyperemia in acute cases . A CT scan can be necessary to specify the fragment size and the importance of displacement if it exists. Two-dimensional or three-dimensional reconstructions can also be performed.
Conservative treatment is generally based on bed rest, non-weight bearing and an effective analgesic treatment . The resumption of weight bearing and physical activities will be gradual. This treatment leads to excellent functional outcome and return to the initial state is usually complete. Massage and active rehabilitation are proscribed before the eighth week because they favour the occurrence of ectopic ossification. Time for recovery varies from two weeks to 4 months. Most patients recover completely without complications after a well-done conservative treatment .
Surgical treatment consists in a reduction of the fracture followed by fixation with screw or pin. It is reserved to fractures with fragment displacement upper to 2 cm and in cases when a short recovery time is desired . For Lafosse et al., such treatment should remain an exception and should be reserved for patients for which early resumption of high activity level is necessary . The main purpose of treatment, whether conservative or surgical, is a return to normal daily life activities and a return to regular sports activities. Complications of conservative treatment are mainly represented by exostoses and nonunion, whereas meralgia paresthetica is the main complication of surgery. Other complications of surgical treatment are sepsis and articular effraction of material .
Preventing these apophyseal avulsions is based on preparatory work to the effort to relax and stretch muscles and on early diagnosis of apophysitis with adequate treatment by immobilization of sufficient duration .
Similarly, when apophysitis is diagnosed in adolescent, other apophyses, which are exposed to great stress, must also be systematically evaluated .
Furthermore, better control by parents of physical activity of children is also important in a society where the sport has become a vehicle for upward social mobility and where athletic performance could lead to physical overload in children and promote lesions of the apophyses .
In conclusion, avulsion fracture of the ASIS is a diagnosis not to ignore in young adults to avoid engaging in an escalation of additional costly and unnecessary tests. The history guides to the diagnosis. Accidents in a sporting context, without any notion of direct impact and with a history of pain, which evoke an old apophysitis, are very evocative. Similarly, diagnosis and early and adapted treatment of growth apophysitis is crucial in preventing the occurrence of such fractures.
Related posts:
 Le Congrès MPR Sofmer 2010 Marseille à l’heure des bilans
Le Congrès MPR Sofmer 2010 Marseille à l’heure des bilans
 Vital and functional outcomes of the first-ever hemispheric stroke, epidemiological comparative study between Kunming (China) and Limoges (France)
Vital and functional outcomes of the first-ever hemispheric stroke, epidemiological comparative study between Kunming (China) and Limoges (France)
 Influence of clinical and gait analysis experience on reliability of observational gait analysis (Edinburgh Gait Score Reliability)
Influence of clinical and gait analysis experience on reliability of observational gait analysis (Edinburgh Gait Score Reliability)
 Cold perception of the bladder during ice water test. Study on 120 patients
Analyse de livre
Cold perception of the bladder during ice water test. Study on 120 patients
Analyse de livre
 A rare case of paraplegia complicating a lumbar epidural infiltration
A rare case of paraplegia complicating a lumbar epidural infiltration
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


