 Anterior Approach to the Ankle
Anterior Approach to the AnkleThe anterior approach provides excellent exposure of the ankle joint for arthrodesis.1 The decision to use this approach rather than the lateral transfibular approach, the medial trans malleolar approach, or the posterior approach depends on the condition of the skin and the surgical technique to be used. Its other uses include the following:
Drainage of infections in the ankle joint
Removal of loose bodies
Open reduction and internal fixation of comminuted distal tibial fractures (pilon fractures)
Position of the Patient
Place the patient supine on the operating table. Partially exsanguinate the foot either by elevating it for 3 to 5 minutes or by applying a soft rubber bandage loosely to the foot and binding it firmly to the calf. Then, inflate a thigh tourniquet. Partial exsanguination allows the neurovascular bundle to be identified, because the venous structures will appear blue. Some continuous vascular oozing must be expected, however (Fig. 1-1).
Landmarks and Incision
Landmarks
The medial malleolus is the bulbous, subcutaneous, distal end of the medial surface of the tibia.
The lateral malleolus is the subcutaneous distal end of the fibula.
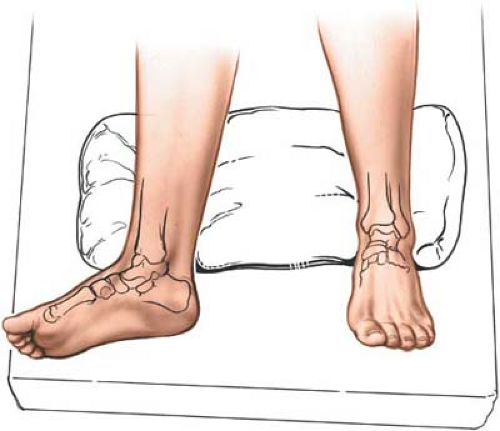 Figure 1-1 Position for the anterior approach to the ankle. |
Incision
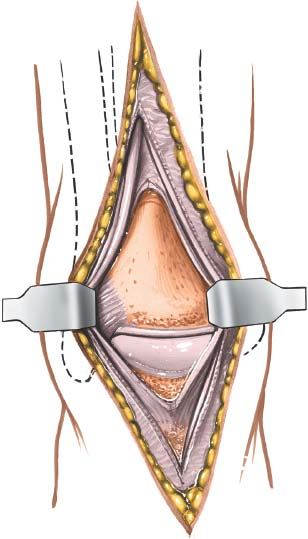
Make a 15-cm longitudinal incision over the anterior aspect of the ankle joint. Begin about 10 cm proximal to the joint, and extend the incision so that it crosses the joint about midway between the malleoli, ending on the dorsum of the foot. Take great care to cut only the skin; the anterior neurovascular bundle and branches of the superficial peroneal nerve cross the ankle joint very close to the line of the skin incision (Fig. 1-2A). Alternatively, make a 15-cm longitudinal incision with its center overlying the anterior aspect of the medial malleolus (see Fig. 1-2).
Internervous Plane
Although the approach uses no true internervous plane, the extensor hallucis longus and extensor digitorum longus muscles define a clear intermuscular plane. Both muscles are supplied by the deep peroneal nerve, but the plane may be used because both receive
their nerve supplies well proximal to the level of the dissection. The plane must be used with great caution, however, because it contains the neurovascular bundle distal to the ankle (see Figs. 25-5 and 25-6).
their nerve supplies well proximal to the level of the dissection. The plane must be used with great caution, however, because it contains the neurovascular bundle distal to the ankle (see Figs. 25-5 and 25-6).
Related posts:
 Lateral Approach to the Lateral Malleolus
Direct Lateral Approach to the Lateral Process of Talus
Hindfoot Nailing for Subtalar and Ankle Joint Fusion (Plantar Approach)
Dorsolateral Approach to Lisfranc’s Joint
Medial Approach to the First Metatarsal Bone for Excision of the Medial Sesamoid Bone
Plantar Approach for Recurrent Morton’s Neuroma
Lateral Approach to the Lateral Malleolus
Direct Lateral Approach to the Lateral Process of Talus
Hindfoot Nailing for Subtalar and Ankle Joint Fusion (Plantar Approach)
Dorsolateral Approach to Lisfranc’s Joint
Medial Approach to the First Metatarsal Bone for Excision of the Medial Sesamoid Bone
Plantar Approach for Recurrent Morton’s Neuroma
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


