 Anterior and Posterior Approaches to the Medial Malleolus
Anterior and Posterior Approaches to the Medial MalleolusThe anterior and posterior approaches are used mainly for open reduction and internal fixation of fractures of the medial malleolus.1 The approaches provide excellent visualization of the malleolus.
Position of the Patient
Place the patient supine on the operating table. The natural position of the leg (slight external rotation) exposes the medial malleolus well. Exsanguinate the limb by elevating it for 3 to 5 minutes, then inflate a tourniquet. Standing or sitting at the foot of the table makes it easier to angle drills correctly (Fig. 3-1).
Incisions
Two skin incisions are available.
The anterior incision offers an excellent view of medial malleolar fractures. It also permits inspection of the anteromedial ankle joint and the anteromedial part of the dome of the talus.
Make a 10-cm longitudinal curved incision on the medial aspect of the ankle, with its midpoint just anterior to the tip of the medial malleolus. Begin proximally, 5 cm above the malleolus and over the middle of the subcutaneous surface of the tibia. Then, cross the anterior third of the medial malleolus, and curve the incision forward to end some 5 cm anterior and distal to the malleolus. The incision should not cross the most prominent portion of the malleolus (Fig. 3-2).
The posterior incision allows reduction and fixation of medial malleolar fractures and visualization of the posterior margin of the tibia.
Make a 10-cm incision on the medial side of the ankle. Begin 5 cm above the ankle on the posterior border of the tibia, and curve the incision downward, following the posterior border of the medial malleolus. Curve the incision forward below the medial malleolus to end 5 cm distal to the malleolus (see Fig. 3-6).
Internervous Plane
No true internervous plane exists in this approach, but the approach is safe because the incision cuts down onto subcutaneous bone.
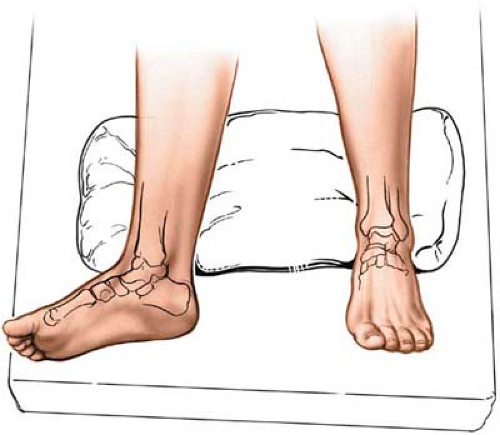 Figure 3-1 Position for the approach to the medial malleolus. The leg falls naturally into a few degrees of external rotation to expose the malleolus. |
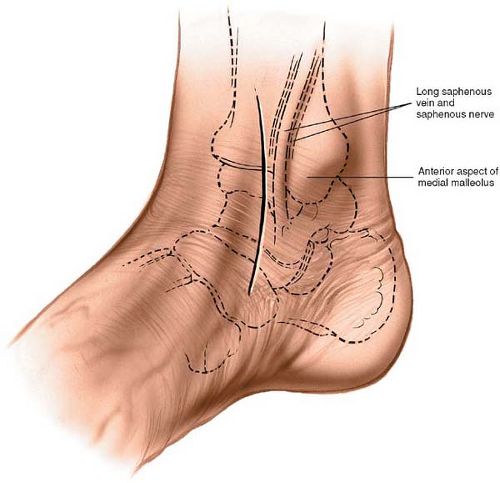 Figure 3-2 Keep the incision just anterior to the tip of the medial malleolus. |
Superficial Surgical Dissection
Anterior Incision
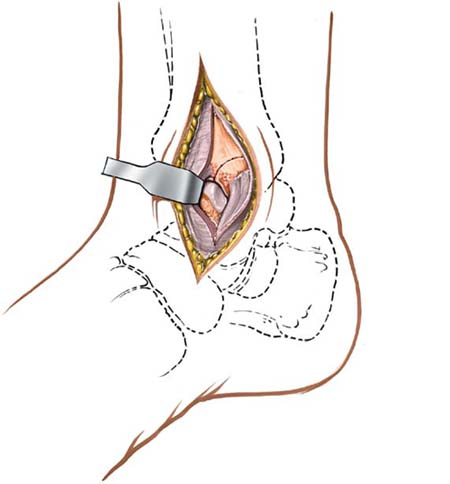
Gently mobilize the skin flaps, taking care to identify and preserve the long saphenous vein, which lies just anterior to the medial malleolus. Accurately locating the skin incision will make it unnecessary to mobilize the skin flaps extensively. Next to the vein runs the saphenous nerve, two branches of which are bound to the vein. Take care not to damage the nerve; damage leads to the formation of a neuroma. Because the nerve is small and not easily identified, the best way to preserve it is to preserve the long saphenous vein, a structure that on its own is of little functional significance (Fig. 3-3).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


