 Ankle Arthroscopy
Ankle ArthroscopyAnkle arthroscopy has become much more popular in the last 10 years. The development of noninvasive distractors and smaller arthroscopes has greatly increased the indications and scope for ankle arthroscopy. The technique was originally used only for diagnostic purposes and removal of loose bodies. More recently, a variety of arthroscopic surgical procedures have become possible. This chapter will describe only the two most commonly used arthroscopic portals: anteromedial and anterolateral. Surgeons wishing to carry out more complex procedures should refer to the original journal articles describing them.
Indications include the following:
Removal of loose bodies or osteochondral fragments
Synovectomy
Removal of soft tissue and osteophytes in case of impingement syndrome
Treatment of osteochondritis dissecans
Microfracture
Ankle arthroscopy has also been used in fracture surgery, both for the removal of chondral loose bodies and assessing the accuracy of reduction.
Three vital structures pass down over the anterior aspect of the ankle: the superficial peroneal nerve; the anterior neurovascular bundle, consisting of the anterior tibial artery and deep peroneal nerve; and the saphenous nerve. Damage to these vital structures should be avoided at all costs. A precise knowledge of their anatomic position is vital in planning incisions used for arthroscopic portals (see Fig. 25-5). A meticulous surgical technique consisting of a skin incision followed by blunt dissection down to the joint capsule is also advised, since the exact position of the structures is subject to anatomic variability.
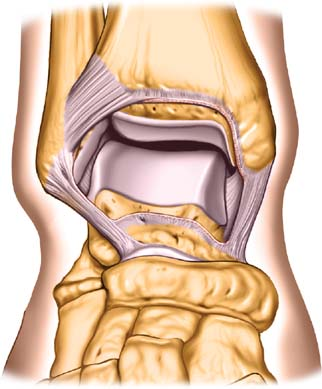
The ankle joint is essentially a hinge joint (ginglymus). The shape of the medial and lateral malleoli together with the strong collateral ligaments allows movement of the ankle in the flexion-extension plane only. The space available within the joint is limited. Distraction of the joint both by external traction and injection of fluid into the joint is therefore necessary for safe insertion of the arthroscope.
Position of the Patient
Place the patient supine on the operating table. Palpate the anterior neurovascular bundle as it runs across the anterior aspect of the ankle joint, just lateral to the tendon of the extensor hallucis longus, and mark its position on the skin. Exsanguinate the limb using a soft rubber bandage, then inflate a mid-thigh tourniquet.
Apply a noninvasive distractor to the dorsum of the foot. Distractors usually consist of a calcaneal component and a dorsal containment strap. If possible, ensure that the calcaneal strap of the distractor is placed so that the foot is elevated. This ensures that you will be able to get access to the posterolateral aspect of the ankle if required during the procedure (Fig. 8-1). Drop the foot of the table 30 degrees to aid access to the anterior aspect of the ankle joint.
Incision and Landmarks
The position of the anterior neurovascular bundle should have already been marked prior to inflation of the tourniquet. Identify the tendon of the tibialis anterior as it runs across the anteromedial aspect of the ankle joint. Finally, flex and extend the ankle to allow you to palpate the joint line with your thumb.
Related posts:
 Posterolateral Approach to the Ankle
Direct Lateral Approach to the Lateral Process of Talus
Hindfoot Nailing for Subtalar and Ankle Joint Fusion (Plantar Approach)
Dorsolateral Approach to Lisfranc’s Joint
Medial Approach to the First Metatarsal Bone for Excision of the Medial Sesamoid Bone
Plantar Approach for Recurrent Morton’s Neuroma
Posterolateral Approach to the Ankle
Direct Lateral Approach to the Lateral Process of Talus
Hindfoot Nailing for Subtalar and Ankle Joint Fusion (Plantar Approach)
Dorsolateral Approach to Lisfranc’s Joint
Medial Approach to the First Metatarsal Bone for Excision of the Medial Sesamoid Bone
Plantar Approach for Recurrent Morton’s Neuroma
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


