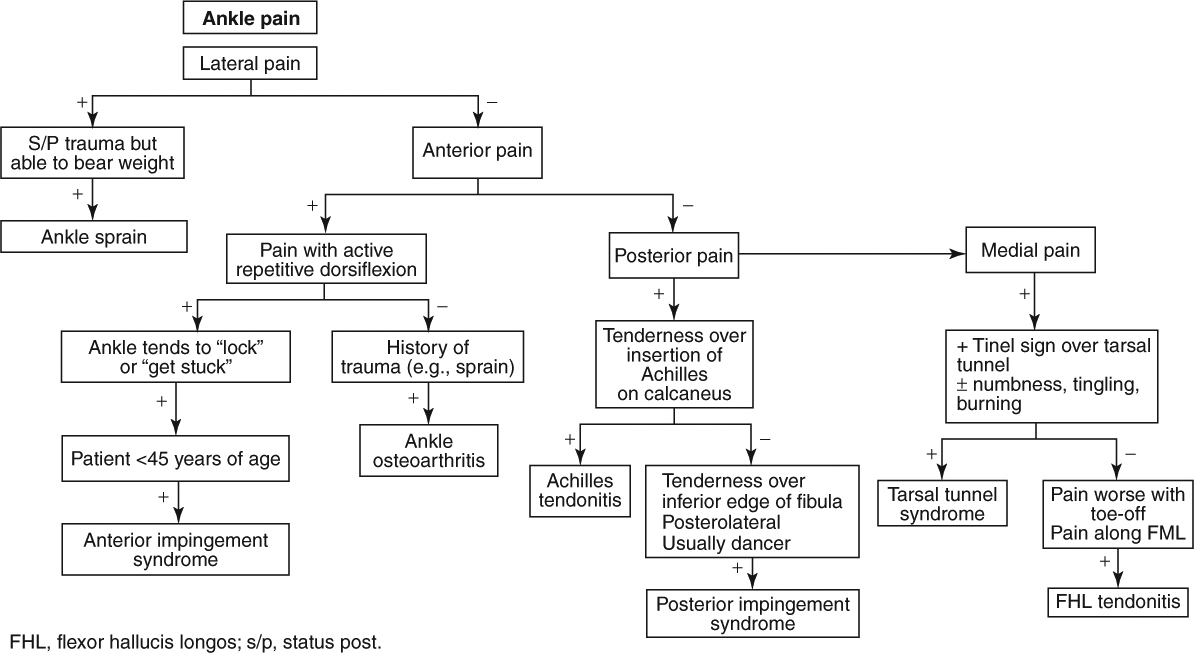
Ankle and Foot Pain
|
Red Flag Signs and Symptoms
Any of these signs and symptoms should prompt urgent evaluation and appropriate intervention:
Fevers
Chills
Hot, swollen joint
Progressive neurologic symptoms
Loss of pulses
ANKLE SPRAIN
Background
Ankle sprains are a very common musculoskeletal problem and account for approximately 75% of injuries to the ankle. They are the most common injury in athletics overall, and they are also relatively common in the general population. The anterior talofibular ligament (ATFL) is the most commonly injured ligament. The calcaneofibular ligament (CFL) is the second most common. The posterior talofibular ligament is only injured in severe sprains.
A grade I sprain indicates a stretching of the ATFL and often also the CFL. A grade II sprain indicates a partial tearing of the ATFL and stretching of the CFL. A grade III sprain indicates a full tearing of the ATFL and CFL and a partial tearing of the PTFL.
The medial deltoid ligament is a strong, dense structure that is rarely injured.
It is important to diagnose and treat ankle sprains appropriately to help prevent chronic ankle instability and pain.
|
Clinical Presentation
Patients generally report an injury in which they “fell over” their foot. On specific questioning, the patient reports the ankle having been in plantar flexion and inversion in the injury. For example, patients may state that they “stumbled over” an inverted foot. At the time of the injury, some patients report hearing a “pop.”
Patients report pain over their lateral ankle. Often, the patient also reports swelling. Weightbearing is difficult (grade I or II) or not possible (grade III) after the injury.
Physical Examination
On examination, ecchymosis and swelling may be present. The involved ligaments are tender. Assess if the patient is able to weight-bear on the involved ankle and how many steps the patient is able to take.
Palpate the medial and lateral malleoli, foot, and fibula and tibia along their entire course.
The anterior drawer and talar tilt test should be performed. In the anterior drawer test (Fig. 8.1), the physician stabilizes the ankle in 20 degrees of plantarflexion with
one hand and with the other hand pulls the calcaneus anteriorly. Excessive anteroposterior glide (in comparison with the asymptomatic side) is considered a positive test and indicates an injury to the ATFL.
one hand and with the other hand pulls the calcaneus anteriorly. Excessive anteroposterior glide (in comparison with the asymptomatic side) is considered a positive test and indicates an injury to the ATFL.
 Figure 8.1 Ankle anterior drawer test. |
In the talar tilt test (Fig. 8.2), the physician inverts the ankle and compares the laxity of the asymptomatic and symptomatic sides. Increased laxity is considered a positive test and indicates an injury to the CFL.
 Figure 8.2 Talar tilt test. |
Diagnostic Studies
The Ottawa ankle rules were developed to help determine which patients with ankle injuries should get radiographs and which ones do not need them. According to a slightly modified version of these rules, if the patient presents within 10 days of injury and is able to bear weight for four steps on the injured ankle and does not have any tenderness in the following areas then the patient does not require radiographs:
Medial and lateral malleoli
Base of the fifth metatarsal
Navicular bone
Posterior inferior 4 inches of the fibula and tibia
If the patient is not able to bear weight on the injured ankle or has pain in any of the areas just listed, however, ankle radiographs, including anteroposterior, lateral, and mortise views, are indicated.
In addition, foot tenderness reveals the need for foot radiographs to rule out a possible concomitant fracture.
Magnetic resonance imaging (MRI) is not routinely indicated. However, if symptoms persist for >6 weeks despite aggressive conservative care, MRI should be considered for further evaluation.
Treatment
First-line treatment for grade I and II sprains includes protection, rest, ice, compression, and elevation (PRICE). Nonsteroidal anti-inflammatory drugs (NSAIDs) can also be taken. Weightbearing should be performed as tolerated. Crutches may be required initially. An air stirrup, brace, or ankle taping is also helpful at first. Patients should return to full gait as tolerated when it is pain free.
Physical therapy is essential and should emphasize early range of motion exercises progressing to proprioceptive and strengthening exercises. Failure to participate fully in an active therapy program may lead to subsequent chronic pain and/or ankle instability.
Patients may return to sport when they can run, jump 10 times on the injured foot, stand for 1 minute on the injured foot with their eyes closed, and pivot on the injured foot without pain.
Patients with a grade III sprain who participate in athletic activities or those who have associated fractures may require surgical intervention.
ACHILLES TENDONITIS (RETROCALCANEAL BURSITIS; HAGLUND SYNDROME)
Background
In the posterior heel, where the Achilles tendon inserts on the calcaneus, are several structures that can cause pain.
The tendon can become fibrotic (tendinosis) and/or inflamed (tendonitis). There is a bursa between the tendon and the skin (pre-Achilles bursa) and a bursa between the tendon and the calcaneus (retrocalcaneal bursa). Both of these bursae can become inflamed (bursitis). In Haglund syndrome, the calcaneus impinges on the Achilles tendon (usually because of a benign overgrowth of the calcaneus, termed the Haglund deformity) and results in Achilles tendonitis and retrocalcaneal bursitis. Even without a Haglund deformity, any of the conditions just described may coexist. Because they are treated very similarly, they are discussed here together.
The tendon can become fibrotic (tendinosis) and/or inflamed (tendonitis). There is a bursa between the tendon and the skin (pre-Achilles bursa) and a bursa between the tendon and the calcaneus (retrocalcaneal bursa). Both of these bursae can become inflamed (bursitis). In Haglund syndrome, the calcaneus impinges on the Achilles tendon (usually because of a benign overgrowth of the calcaneus, termed the Haglund deformity) and results in Achilles tendonitis and retrocalcaneal bursitis. Even without a Haglund deformity, any of the conditions just described may coexist. Because they are treated very similarly, they are discussed here together.
When younger patients (between 10 and 14 years of age) complain of posterior heel pain, they may have Sever disease. This is believed to be an overuse injury in the setting of a tight Achilles tendon, which results in a retrocalcaneal apophysitis (where the Achilles tendon attaches to the calcaneus).
Clinical Presentation
Patients typically complain of posterior heel pain (anywhere from 2 inches above the calcaneus to the calcaneus) that is exacerbated by activities such as walking and running. Often, women report wearing high-heeled shoes. In children, the pain typically begins at the beginning of a new sport season.
Physical Examination
The hallmark examination finding is tenderness over, around, or immediately anterior to the Achilles tendon as it inserts on the calcaneus. The Achilles tendon is also often found to be tight. A small effusion may be present.
Diagnostic Studies
Radiographs may be ordered to rule out bony abnormality, including the Haglund deformity. In older patients, calcifications of the Achilles tendon may be seen.
Treatment
Rest, ice, compression, and elevation (RICE) is the cornerstone of initial treatment. Activities should be modified so they are not painful. A heel lift may be used temporarily to minimize pressure. Importantly, the patient should begin a physical therapy program that emphasizes stretching the Achilles tendon. Occasionally, casting may be used to reduce movement of the tendon. NSAIDs may also be helpful.
Injections should not be performed in this area because of the risk of rupturing the Achilles tendon.
In the case of the Haglund deformity, surgical excision of the bony overgrowth may be required in patients who do not respond to more conservative therapy.
Sever disease is also treated conservatively. Patients usually respond well to RICE and physical therapy. Patients can return to sports once they are pain free and have improved their ankle flexibility. They should continue an Achilles stretching program and icing to help prevent further problems once back at athletics.
ANKLE OSTEOARTHRITIS
Background
Patients with ankle osteoarthritis (OA) typically have a history of trauma to the ankle joint. Ankle OA in general is not as common as OA in other areas of the body. If a history of trauma is not present, rheumatoid arthritis should be more expected.
Clinical Presentation
Patients typically present with gradually increasing pain in the ankle joint. On questioning, they usually relate a history of ankle trauma that may have occurred in the distant past. Patients may also complain of ankle stiffness and swelling. The pain is typically primarily in the anterior ankle. Weightbearing exacerbates the pain.
Physical Examination
Patients may walk with an antalgic gait in which they favor the unaffected side. A mild effusion of the ankle may be present. Passive range of motion may reproduce pain. Range of motion is also often reduced.
Diagnostic Studies
Weightbearing radiographs should be obtained.
Treatment
RICE, physical therapy, and NSAIDs are appropriate first-line treatment for ankle OA. In addition, an intra-articular steroid injection, preferably performed under ultrasound or fluoroscopic guidance, can be very helpful.
Research is promising but still ongoing into the potential use of intra-articular hyaluronic acid injections for ankle OA.
Occasionally, an ankle-foot orthosis (AFO) can be used to allow the ankle joint to rest after an acute flare-up of OA. However, if an AFO is used, exercises should be continued to maintain flexibility within the joint.
When aggressive conservative care is insufficient, surgical options include ankle arthrodesis and total ankle replacement.
TARSAL TUNNEL SYNDROME
Background
The tarsal tunnel is located posterior to the medial malleolus. Through it pass the posterior tibial nerve, posterior tibial artery, and tendons of the tibialis posterior, flexor digitorum longus, and flexor hallucis longus. The mnemonic “Tom, Dick, and Harry” is sometimes used to remember these structures.
Compression of the posterior tibial nerve within the tarsal tunnel can occur as a result of biomechanical causes, a ganglion, bony lesion, trauma, or idiopathic reasons.
Clinical Presentation
Patients typically present with vague symptoms of diffuse medial ankle pain. Paresthesias, including burning, tingling, and/or numbness, commonly occur over the medial ankle over the tunnel and radiate into the arch of the foot. Patients generally report that the symptoms are worse with running and other activities and better with rest. Nighttime pain is also not uncommon. Occasionally, the pain and paresthesias may radiate proximally into the distal lower leg.
Physical Examination
The classic finding is reproduction of symptoms while tapping over the tunnel (Tinel test). In severe cases, atrophy of the intrinsic muscles may be observed. Numbness may be detected over the medial and posterior calcaneus and/or arch of the foot. While observing the patient’s gait, hyperpronation may be present.
Diagnostic Studies
Radiographs should be obtained to rule out bony abnormalities. An MRI is helpful to determine a structural cause of the symptoms. Ultrasound can also be used for this purpose.
Electromyelography/nerve conduction velocity studies are helpful to confirm the diagnosis and rule out other potential pathologies.
Treatment
If the patient is hyperpronating, an orthotic is helpful to correct this problem. A steroid and anesthetic injection into the tunnel (preferably done under ultrasound guidance to ensure accurate placement and avoidance of injecting the nerve or tendon) can be effective.
When aggressive conservative care does not adequately eliminate the symptoms, surgical decompression may be necessary. If a structural lesion is identified, it can be
removed. If adhesions are observed on the nerve, this may be contributing to its entrapment, in which case external neurolysis may be helpful. If no structural lesion is identified on imaging, however, surgery is not as likely to be successful.
removed. If adhesions are observed on the nerve, this may be contributing to its entrapment, in which case external neurolysis may be helpful. If no structural lesion is identified on imaging, however, surgery is not as likely to be successful.
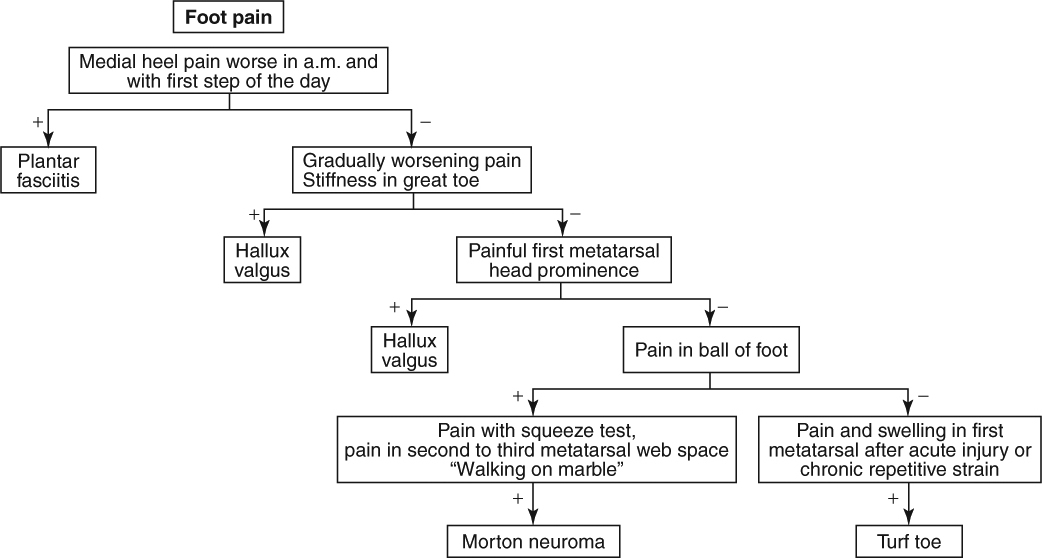
HALLUX RIGIDUS
Background
Hallux rigidus, which translates to “stiff great toe,” refers to osteoarthritis (OA) of the first metatarsal phalangeal (MTP) joint. It is believed to be primarily a disease of overuse from repetitive wear and tear and hyperextension. It is most common in patients 30 to 60 years of age but may occur as early as adolescence.
Clinical Presentation
Patients generally present with complaints of pain and stiffness in their great toe. Running and other weightbearing activities tend to exacerbate the pain. Patients may note that toe-off during gait is particularly painful. If the symptoms have been present for an extended period of time, altered biomechanics may have led the patient to develop pain in the lateral aspect of the foot and/or knee. Tight shoes also exacerbate the pain.
Physical Examination
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


