Anatomy of the Shoulder and Elbow
Jonathan Barlow
Matthew L. Ramsey
Gerald R. Williams Jr.
Joseph A. Abboud
OVERVIEW OF SHOULDER AND ELBOW SURGERY
In order to diagnose and treat problems of the shoulder and elbow, one must fully understand the anatomy of the region and appreciate how this translates to functional derangements.
There is no line of demarcation between the shoulder and elbow regions. Pain in the arm may originate at the neck or shoulder and refer down the arm. Less often, pain noted by patients at the elbow or forearm has local origin. If the slightest doubt exists as to the etiology of the pain, the patient is examined from neck to fingers.
The upper extremity functions to position and move the hand in space. The upper extremities are attached to the body by the sternoclavicular joint. Otherwise, they are suspended from the neck and held fast to the torso by soft tissues (muscles and fascia).
The upper extremity gains leverage against the posterior aspect of the thorax by virtue of the broad, flat body of the scapula.
The elbow is a complex modified hinge articulation. Unlike the shoulder, the elbow has much more intrinsic stability based on its bony architecture. The primary purpose of the elbow is to position the hand in space.
An increasing knowledge of the pathoanatomy and biomechanics of the shoulder and elbow has guided development of new and innovative surgical techniques and devices that have allowed more effective treatment of a number of disorders.
Arthroscopic surgery, in particular, has significantly increased our ability to surgically manage conditions and reduce morbidity. The Sports Medicine portion of this textbook handles the arthroscopic management of shoulder and elbow disorders.
The art of any surgery lies in the reconstruction of diseased or injured tissues with minimal additional destruction. Skillful handling of the soft tissues is the hallmark of all upper extremity surgery, including surgery about the shoulder and elbow. Knowledge of anatomy defines the precision and safety of surgery. Approaches to any joint in the body are developed on this foundation, with particular emphasis on the exploitation of internervous planes. Familiarity with the intricate anatomy and multiple approaches to the shoulder and elbow allows the surgeon to confidently embark on the repair or reconstruction of the injury or disorder of the joint.
ANATOMY OF THE SHOULDER
The shoulder has the greatest mobility of any joint in the body and therefore the greatest predisposition to dislocation.
This great range of motion is distributed to three diarthrodial joints: the glenohumeral, the acromioclavicular, and the sternoclavicular.
The last two joints, in combination with the fascial spaces between the scapula and the chest, are known collectively as the scapulothoracic articulation.
OSTEOLOGY
Clavicle
This is a relatively straight bone when viewed anteriorly, whereas in the transverse plane, it resembles an italic S (FIG 1).
There are three bony impressions for ligament attachment to the clavicle:
On the medial side is an impression for the costoclavicular ligament, which at times may be a rhomboid fossa.
At the lateral end of the bone is the conoid tubercle.
Just lateral to the conoid tubercle is the trapezoid tubercle.
Muscles that insert on the clavicle are the trapezius on the posterosuperior surface of the distal end and the subclavius muscle, which has an insertion on the inferior surface of the middle third of the clavicle.
The clavicle serves as a site of muscular attachment and a strut for the shoulder girdle.
Although historical literature discussed the clavicle as predominantly as a site of muscular attachment, recent work, especially regarding displaced clavicle fractures, has demonstrated an important structural function of the clavicle as a strut for the shoulder girdle, maintaining the position of the scapulothoracic articulation and glenohumeral joint in space.
Four muscles take origin from the clavicle: deltoid, pectoralis major, sternocleidomastoid, and sternohyoid.
Important relations to the clavicle are the subclavian vein and artery and the brachial plexus inferiorly.
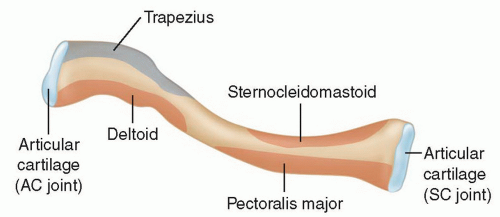 FIG 1 • The clavicle. AC, acromioclavicular; SC, sternoclavicular. |
Scapula
This is a thin sheet of bone that functions mainly as a site of muscle attachment (FIG 2A).
It is thicker at its superior and inferior angles in its lateral border, where some of the more powerful muscles are attached.
It is also thick in forming its processes: coracoid, spine, acromion, and glenoid.
The coracoid process comes off the scapula at the upper base of the neck of the glenoid and passes anteriorly before hooking to a more lateral position.
Functions as the origin of the short head of the biceps and the coracobrachialis tendons
Serves as the insertion of the pectoralis minor muscle and the coracoacromial, coracohumeral, and coracoclavicular ligaments
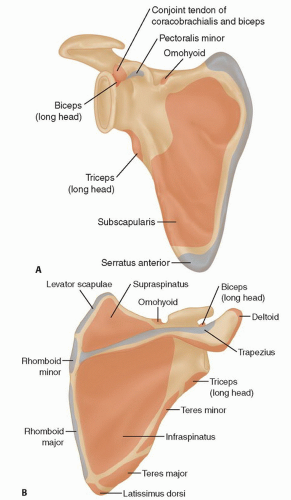
FIG 2 • A. The scapula. B. The supraspinatus and infraspinatus fossa.
The spine of the scapula functions as part of the insertion of the trapezius on the scapula as well as the origin of the posterior deltoid.
Also serves to suspend the acromion in the lateral and anterior directions to serve as a prominent lever arm for function of the deltoid
The posterior surface of the scapula and the presence of the spine create the supraspinatus and infraspinatus fossa (FIG 2B).
The acromion is the most studied process of the scapula because of the amount of pathology involving the acromion and the rotator cuff.
Type 1, with its flat surface, provided the least compromise of the supraspinatus outlet, whereas type 3, which has a hook, was associated with the highest rate of rotator cuff pathology in a series of cadaver dissections.
The glenoid articular surface is within 10 degrees of being perpendicular to the blade of the scapula, with the mean being 6 degrees of retroversion.
More caudad portions face more anteriorly than cephalad.
Three processes—the spine, the coracoid, and the glenoid— create two notches in the scapula.
Suprascapular notch is at the base of the coracoid.
Spinoglenoid, or greater scapular notch, is at the base of the spine.
Major ligaments that take origin from the scapula are as follows:
Coracoclavicular
Coracoacromial
Acromioclavicular
Glenohumeral
Coracohumeral
Blood supply to the scapula derives from vessels in the muscles that take fleshy origin from the scapula.
Vessels cross these indirect insertions and communicate with bony vessels.
Humerus
The articular surface of the humerus at the shoulder is spheroid, with a radius of curvature of about 2.25 cm.
With the arm in the anatomic position (ie, with the epicondyles of the humerus in the coronal plane), the head of humerus has retroversion of about 30 degrees, with a wide range of normal values.
The intertubercular groove lies about 1 cm lateral to the midline of the humerus (FIG 4).
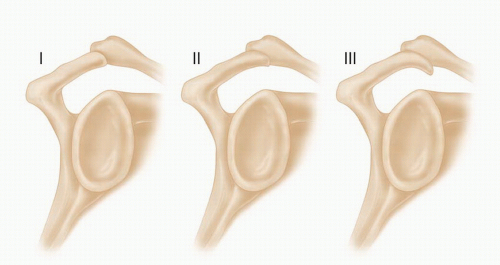
FIG 3 • Acromion morphologies.
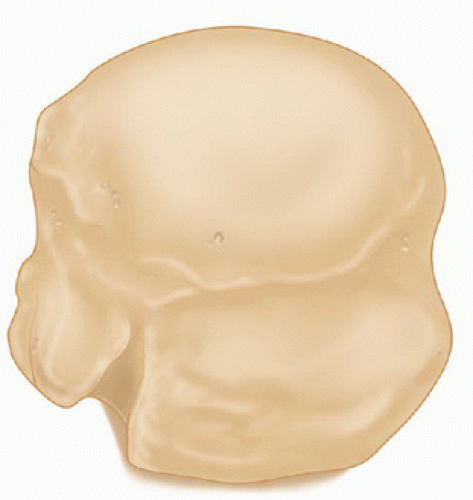
FIG 4 • The humerus.
The axis of the humeral head crosses the greater tuberosity at about 9 mm posterior to the bicipital groove.
The lesser tuberosity lies directly anterior, and the greater tuberosity lines up on the lateral side.
The lesser tuberosity is the insertion for the subscapularis tendon.
The greater tuberosity bears the insertion of the supraspinatus, infraspinatus, and teres minor in a superior to inferior order.
Greater and lesser tuberosities make up the boundaries of the intertubercular groove through which the long head of the biceps passes from its origin on the superior lip of the glenoid.
The intertubercular groove has a peripheral roof referred to as the intertubercular ligament or the transverse humeral ligament, which has varying degrees of strength.
In the coronal plane, the head-shaft angle is about 135 degrees.
The space between the articular cartilage and the ligamentous and tendon attachments is referred to as the anatomic neck of the humerus.
Below the level of the tuberosities, the humerus narrows in a region that is referred to as the surgical neck of the humerus because of the frequent occurrence of fractures at this level.
Historically, the humeral head was thought to be perfused predominantly by the ascending branch of the anterior humeral circumflex artery, traveling along the biceps groove. Recent work, however, has demonstrated that the posterior humeral circumflex artery has a vital function in perfusing the humeral head.
STERNOCLAVICULAR JOINT
This is the only skeletal articulation between the upper limb and the axial skeleton.
Ligaments
The major ligaments of the sternoclavicular joint are the anterior and posterior sternoclavicular ligaments.
The most important ligament of this group, the posterior sternoclavicular ligament, is the strongest.
Blood Supply
Blood supply of the sternoclavicular joint derives from the clavicular branch of the thoracoacromial artery, with additional contributions from the internal mammary and the suprascapular arteries.
Nerve Supply
Arises from the nerve to the subclavius, with some contribution from the medial suprascapular artery
ACROMIOCLAVICULAR JOINT
Only articulation between the clavicle and the scapula
Ligaments
Ligaments about the acromioclavicular articulation include the superior and inferior acromioclavicular ligaments and the coracoclavicular ligaments (the trapezoid and the conoid ligaments (FIG 5).
The anteroposterior stability of the acromioclavicular joint is controlled by the acromioclavicular ligaments, and the vertical stability is controlled by the coracoclavicular ligaments.
Blood Supply
Blood supply derives mainly from the acromial artery, a branch of the deltoid artery of the thoracoacromial axis.
There are rich anastomoses between the thoracoacromial artery, suprascapular artery, and posterior humeral circumflex artery.
The acromial artery comes on to the thoracoacromial axis anterior to the clavipectoral fascia and perforates back through the clavipectoral fascia to supply the joint.
Nerve Supply
Innervation of the joint is supplied by the lateral pectoral, axillary, and suprascapular nerves.
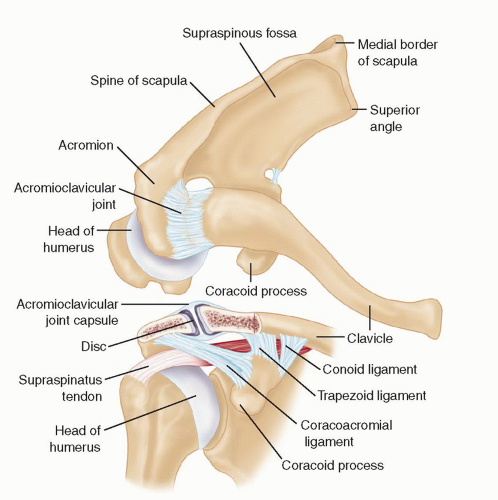 FIG 5 • Acromioclavicular joint. |
SHOULDER LIGAMENTS: CAPSULOLIGAMENTOUS AND LABRAL ANATOMY
Superior Glenohumeral Ligament
Arises near the origin of the long head of the biceps brachii
If the glenoid had the markings of a clock, with the 12 o’clock position superiorly and the 3 o’clock position anteriorly, the origin of the superior glenohumeral ligament (SGHL) would correspond to the area from the 12 o’clock to the 2 o’clock positions (FIG 6).
SGHL runs inferiorly and laterally to insert on the humerus, superior to the lesser tuberosity.
Middle Glenohumeral Ligament
Usually arises from the neck of the glenoid just inferior to the origin of the SGHL and inserts into the humerus just medial to the lesser tuberosity. Arthroscopically, it can be easily identified as it crosses the superior boarder of the subscapularis at a 90-degree angle.
Presence of the middle glenohumeral ligament (MGHL) is the most variable of any shoulder ligament.
Inferior Glenohumeral Ligament
Most important ligament for providing anterior and posterior shoulder stability
Inferior glenohumeral ligament (IGHL) has been described as having an anterior and posterior band, with an axillary pouch between the bands.
With abduction and external rotation, the anterior band fans out and the posterior band becomes cordlike.
Likewise, with internal rotation, the posterior band fans out and the anterior band appears cordlike.
Anterior band of the IGHL arises from various areas corresponding to the 2 o’clock to 4 o’clock positions on the glenoid.
Insertion site of this ligament has two attachments, one to the glenoid labrum and the other directly to the anterior neck of the glenoid.
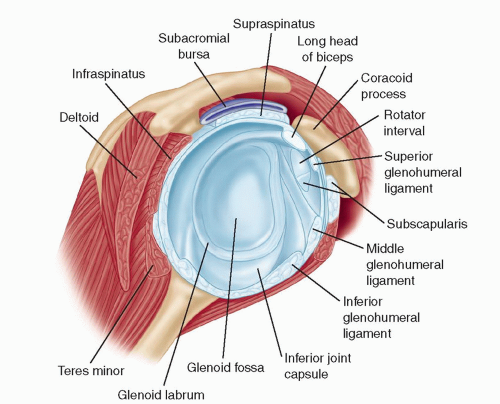
FIG 6 • Shoulder ligaments.
Posterior band originates at the 7 o’clock to 9 o’clock positions.
With the arm at the side, both the anterior and the posterior bands pass through a 90-degree arc and insert on the humerus.
Labrum
Surrounds the periphery of the glenoid and is a site of attachment of the capsuloligamentous structures
It is composed of dense fibrous connective tissue, with a small fibrocartilaginous transition zone at the anteroinferior attachment of the osseous glenoid rim.
The labrum acts as a load-bearing structure for the humeral head and serves to increase the surface area of the glenoid.
Howell and Galinat2 showed that the labrum deepened the glenoid socket by nearly 50%.
Lippitt and coworkers3 have shown that removal of the labrum decreases the joint’s stability to sheer stress by 20%.
Triangular cross-section of the labrum allows it to act as a chock-block to help prevent subluxation.
SCAPULOTHORACIC MUSCLES
Trapezius
Largest and most superficial of scapulothoracic muscles
Takes origin from spinous process of C7-T12 vertebrae
Insertion of the upper fibers is over the distal one-third of the clavicle.
Lower cervical and upper thoracic fibers of the trapezius have their insertion over the acromion and spinous scapula.
Lower portion of the muscle takes insertion at the base of the scapular spine.
Acts as a scapular retractor, with the upper fibers used mostly for elevation of the lateral angle
Spinal accessory nerve is the motor supply.
Arterial supply is derived from transverse cervical artery.
Rhomboids
Similar in function to the midportion of the trapezius, with origin from the lower ligamentum nuchae, C7 and T1 for the rhomboid minor, and T2-T5 for the rhomboid major
Rhomboid minor inserts on the posterior portion of the medial base of the spine of the scapula.
Rhomboid major inserts to the posterior surface of the medial border, from where the minor leaves off down to the inferior angle of the scapula.
Action of the rhomboids is retraction of the scapula, and because of their oblique course, they also participate in elevation of the scapula.
Innervation is the dorsal scapular nerve (C5), which may arise off the brachial plexus in common with the nerve to the subclavius or with the C5 branches of the long thoracic nerve.
Dorsal scapular artery provides arterial supply to the muscles through their deep surfaces.
Levator Scapula and Serratus Anterior
The levator scapula and the serratus anterior are often discussed together because of their close relationship anatomically and functionally.
The levator scapula takes origin from the posterior tubercles of the transverse process from C1 through C3 and sometimes C4.
Inserts on the superior angle of the scapula
Acts to elevate the superior angle of the scapula
In conjunction with the serratus anterior, produces upward rotation of the scapula
Innervation is from the deep branches of C3 and C4.
Serratus anterior takes origin from the ribs on the anterior lateral wall of the thoracic cage.
Bounded medially by the ribs and intercostal muscles and laterally by the axillary space
Protracts the scapula and participates in upward rotation of the scapula
More active in flexion than in abduction because straight abduction requires some retraction of the scapula
Absence of serratus activity, usually because of paralysis, produces a winging of the scapula with forward flexion of the arm and loss of strength in that motion.
Innervation is supplied by the long thoracic nerve (C5-C7).
Blood supply is from the lateral thoracic artery, with a large contribution from the thoracodorsal artery.
Pectoralis Minor
Takes fleshy origin anteriorly on the chest wall, and second through fifth ribs, and has its insertion onto the base of the medial side of the coracoid
Function is protraction of the scapula if the scapula is retracted and depression of the lateral angle or downward rotation of the scapula if the scapula is upwardly rotated.
Innervation is from the medial pectoral nerve (C8 and T1).
Blood supply is through the pectoral branch of the thoracoacromial artery.
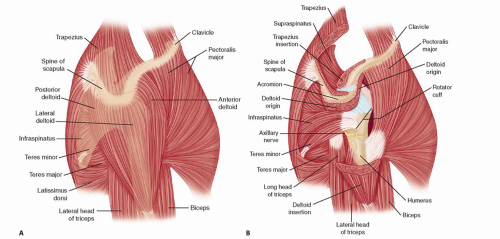 FIG 7 • A,B. Glenohumeral muscles. |
GLENOHUMERAL MUSCLES
Deltoid
Largest and most important of the glenohumeral muscles, consisting of three major sections:
Anterior deltoid takes origin off the lateral third of the clavicle, middle third of the deltoid takes origin off the acromion, and posterior deltoid takes origin from the spine of the scapula (FIG 7).
The deltoid is supplied by the axillary nerve (C5 and C6), which enters the posterior portion of the shoulder through the quadrilateral space and innervates the teres minor in this position.
Nerves to the posterior third of the deltoid enter the muscle very close to their exit from the quadrilateral space, traveling in the deltoid muscle along the medial and inferior borders of the posterior deltoid.
Branch of the axillary nerve that supplies the anterior two-thirds of the deltoid ascends superiorly and then travels anteriorly, about 5 cm inferior to the rim of the acromion.
Vascular supply to the deltoid is largely derived from the posterior humeral circumflex artery, which travels with the axillary nerve through the quadrilateral space and on the deep surface of the muscle.
Deltoid is also supplied by the deltoid branch of the thoracoacromial artery.
Supraspinatus
Lies on the superior portion of the scapula
It takes origin from the supraspinatus fossa and overlying fascia and inserts into the greater tuberosity.
Its tendinous insertion is in common with the infraspinatus posteriorly.
It is active in any motion involving elevation.Related posts:
 Management of Glenohumeral Instability with Humeral Bone Loss
Subscapularis Repair, Coracoid Recession, and Biceps Tenodesis
Acute Repair and Reconstruction of Sternoclavicular Dislocation
Reverse Shoulder Arthroplasty for Proximal Humerus Fractures
Pectoralis Major Repair
Eden-Lange Procedure for Trapezius Palsy
Management of Glenohumeral Instability with Humeral Bone Loss
Subscapularis Repair, Coracoid Recession, and Biceps Tenodesis
Acute Repair and Reconstruction of Sternoclavicular Dislocation
Reverse Shoulder Arthroplasty for Proximal Humerus Fractures
Pectoralis Major Repair
Eden-Lange Procedure for Trapezius Palsy

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


