Eating and swallowing are complex behaviors involving volitional and reflexive activities of more than 30 nerves and muscles. They have two crucial biologic features: food passage from the oral cavity to stomach and airway protection. The swallowing process is commonly divided into oral, pharyngeal, and esophageal stages, according to the location of the bolus. The movement of the food in the oral cavity and to the oropharynx differs depending on the type of food (eating solid food versus drinking liquid). Dysphagia can result from a wide variety of functional or structural deficits of the oral cavity, pharynx, larynx, or esophagus. The goal of dysphagia rehabilitation is to identify and treat abnormalities of feeding and swallowing while maintaining safe and efficient alimentation and hydration.
Anatomy
Anatomy of structures
Understanding the normal physiology and pathophysiology of eating and swallowing is fundamental to evaluating and treating disorders of eating and swallowing and to developing dysphagia rehabilitation programs. Eating and swallowing are complex behaviors that include volitional and reflexive activities involving more than 30 nerves and muscles .
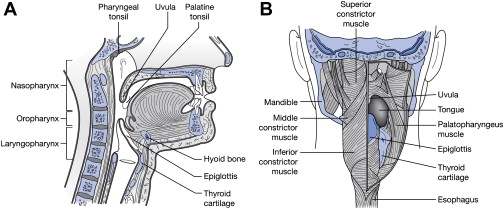
Fig. 1 shows the anatomy of the oral cavity, pharynx, and larynx; Table 1 lists the innervation of the major muscles related to swallowing. The tongue has oral and pharyngeal surfaces. The oral cavity is separated from the pharynx by the faucial pillars. The pharynx has a layer of constrictor muscles that originate on the cranium and hyoid bone and the thyroid cartilage anteriorly, and insert on a posterior median raphe. The submental muscles originate on the mandible and attach to the hyoid bone and tongue. The cricopharyngeus muscle is attached to the sides of the cricoid cartilage anteriorly and closes the upper esophageal sphincter (UES) by compressing it against the back of the cricoid cartilage. The epiglottis originates in the larynx and is angled upward and backward. It is attached to the hyoid bone anteriorly. The space between the pharyngeal surface of the tongue and the epiglottis is called the valleculae. The larynx includes the true and false vocal folds and the laryngeal surface of the epiglottis. The laryngeal aditus (upper end of the larynx) opens into the lower portion of the pharynx. Lateral to the larynx are two spaces in the pharynx called the pyriform recesses.
| Cranial nerves | Muscles |
|---|---|
| Trigeminal nerve (V) |
|
| Facial nerve (VII) |
|
| Glossopharyngeal nerve (IX) | Stylopharyngeus |
| Vagus nerve (X) |
|
| Hypoglossal nerve (XII) |
|
Development of anatomy
The anatomy of the head and neck in infants is different from that in adults. In the infant, teeth are not erupted, the hard palate is flatter, and the larynx and hyoid bone are higher in the neck to the oral cavity. The epiglottis touches the back of the soft palate so that the larynx is open to the nasopharynx, but this airway is separated from the oral cavity by a soft tissue barrier ( Fig. 2 ). The anatomy of the pharynx in humans changes with development. As the neck gets longer, the larynx descends to a position lower in the neck. The contact of the soft palate and epiglottis is lost, and the pharynx becomes longer vertically. This change in human development contributes to the development of speech, but because the pharynx becomes part of the food passageway and the airway (see Fig. 2 ), humans are vulnerable for aspiration.

Physiology
Two paradigmatic models are commonly used to describe the physiology of normal eating and swallowing: the four-stage model for drinking and swallowing liquid and the process model for eating and swallowing solid food. The normal swallow in humans was originally described using a three-stage sequential model whereby the swallowing process was divided into oral, pharyngeal, and esophageal stages according to the location of the bolus . The oral stage was later subdivided into the oral-preparatory and oral-propulsive stages, thus establishing the four-stage model. Studies based on the four-stage model adequately describe the biomechanics and bolus movement during command swallows of liquids; however, this model cannot represent the bolus movement and the process of eating of solid food. Therefore, the process model of feeding was established to describe the mechanism of eating and swallowing solid food .
Oral-preparatory stage
After liquid is taken into the mouth from a cup or through a straw, the liquid bolus is held in the anterior part of the floor of the mouth or on the tongue surface against the hard palate surrounded by the upper dental arch (upper teeth). The oral cavity is sealed posteriorly by the contact between the soft palate and the tongue to prevent the liquid bolus from leaking into the oropharynx before the swallow. There may be leakage of liquid into the pharynx when the seal is imperfect, and this leakage increases with aging.
Oral-propulsive stage
During the oral-propulsive stage, the tongue tip rises, touching the alveolar ridge of the hard palate just behind the upper teeth, while the posterior tongue drops to open the back of the oral cavity. The tongue surface moves upward, gradually expanding the area of tongue–palate contact from anterior to posterior, squeezing the liquid bolus back along the palate and into the pharynx. When drinking liquids, the pharyngeal stage normally begins during oral propulsion.
Oral stage in eating solid food (process model of feeding)
The four-stage sequential model has limited utility for describing the process of normal eating in humans, especially that of food transport and bolus formation in the oropharynx . When healthy subjects eat solid food, triturated (chewed and moistened) food commonly passes through the fauces for bolus formation in the oropharynx (including the valleculae) several seconds before the pharyngeal stage of a swallow. Additional portions of food can pass into the oropharynx and accumulate there while food remains in the oral cavity and chewing continues. This phenomenon is not consistent with the four-stage model because of the overlap among the oral-preparatory, oral-propulsive, and pharyngeal stages; the observable events during feeding on solid food are better described with the process model of feeding, which has its origin in studies of mammalian feeding and was later adapted to feeding in humans .
Stage I transport
When food is ingested into the mouth, the tongue carries the food to the postcanine region and rotates laterally, placing the food onto the occlusal surface of lower teeth for food processing.
Food processing
Food processing immediately follows stage I transport. During food processing, food particles are reduced in size by mastication and are softened by salivation until the food consistency is optimal for swallowing. Chewing continues until all of the food is prepared for swallowing. Cyclic movement of the jaw in processing is tightly coordinated with the movements of the tongue, cheek, soft palate, and hyoid bone ( Fig. 3 ).
During drinking of liquid, the posterior oral cavity is sealed by tongue–palate contact during the oral-preparatory stage when the bolus is held in the oral cavity. In contrast, during food processing, the tongue and soft palate move cyclically in association with jaw movement, permitting open communication between the oral cavity and pharynx . Therefore, there is no sealing of the posterior oral cavity during eating. Movements of the jaw and tongue pump air into the nasal cavity through the pharynx, delivering the food’s aroma to chemoreceptors in the nose .
Cyclic tongue movement during processing is coordinated with jaw movement . Tongue movements during processing are large in the anteroposterior and vertical dimensions; jaw movements are similarly large in the vertical dimension (see Fig. 3 A). During jaw opening, the tongue moves forward and downward, reaching its most anterior point in mid to late jaw opening. It then reverses direction and moves backward in late jaw opening, preventing us from biting our tongues when we eat. The tongue also moves medioalaterally and rotates on its long (anteroposterior) axis during chewing . These motions are coordinated with cheek movement to keep food on the occlusal surfaces of the lower teeth. The hyoid bone also moves constantly during feeding, but its motion is more variable than jaw or tongue movements (see Fig 3 A and B). The hyoid has mechanical connections to the cranial base, mandible, sternum, and thyroid cartilage by way of the suprahyoid and infrahyoid muscles. With those muscle connections, the hyoid plays an important role in controlling the movements of the jaw and tongue.
Stage II transport
When a portion of the food is suitable for swallowing, it is placed on the tongue surface and propelled back through the fauces to the oropharynx ( Fig. 4 ). The basic mechanism of stage II transport is the same as described for the oral-propulsive stage with a liquid bolus. The anterior tongue surface first contacts the hard palate just behind the upper incisors. The area of tongue–palate contact gradually expands backward, squeezing the triturated food back along the palate to the oropharynx. Stage II transport is primarily driven by the tongue and does not require gravity . Stage II transport can be interposed into food processing cycles. The transported food accumulates on the pharyngeal surface of the tongue and in the valleculae. Chewing continues when food remains in the oral cavity, and the bolus in the oropharynx is enlarged by subsequent stage II transport cycles. The duration of bolus aggregation in the oropharynx ranges from a fraction of a second to about 10 seconds in normal individuals eating solid food .
Pharyngeal stage
Pharyngeal swallow is a rapid sequential activity, occurring within a second. It has two crucial biologic features: (1) food passage—propelling the food bolus through the pharynx and UES to the esophagus; and (2) airway protection—insulating the larynx and trachea from the pharynx during food passage to prevent the food from entering the airway.
During the pharyngeal stage, the soft palate elevates and contacts the lateral and posterior walls of the pharynx, closing the nasopharynx at about the same time that the bolus head comes into the pharynx ( Fig. 5 ). Soft palate elevation prevents bolus regurgitation into the nasal cavity. The base of the tongue retracts, pushing the bolus against the pharyngeal walls (see Fig. 5 ). The pharyngeal constrictor muscles contract sequentially from the top to the bottom, squeezing the bolus downward. The pharynx also shortens vertically to reduce the volume of the pharyngeal cavity.
Safe bolus passage in the pharynx without aspirating food is critical in human swallowing. There are several airway protective mechanisms preventing aspiration of the foreign materials to the trachea before or during swallowing. The vocal folds close to seal the glottis (space between the vocal folds), and the arytenoids tilt forward to contact the epiglottic base before opening of the UES . The hyoid bone and larynx are pulled upward and forward by contraction of the suprahyoid muscles and thyrohyoid muscle. This displacement tucks the larynx under the base of the tongue. The epiglottis tilts backward to seal the laryngeal vestibule. The mechanism of the epiglottic tilting in human swallowing remains unclear but is probably related to hyolaryngeal elevation, pharyngeal constriction, bolus movement, and tongue-base retraction .
Opening of the UES is essential for the bolus entry into the esophagus. The UES consists of the inferior pharyngeal constrictor muscles, cricopharyngeous muscle, and the most proximal part of the esophagus. The UES is closed at rest by tonic muscle contraction . Three important factors contribute to UES opening: (1) relaxation of the cricopharyngeous muscle—this relaxation normally precedes opening of the UES or arrival of the bolus; (2) contraction of the suprahyoid muscles and thyrohyoid muscles—these muscles pull the hyolaryngeal complex forward, opening the sphincter; and (3) the pressure of the descending bolus—this pressure distends the UES, assisting its opening . The most important of these mechanisms is the active opening process, making the opening of the UES different from other sphincters such as the external urethral sphincter, which opens passively (the urethral sphincter relaxes and is pushed open by the descending fluid bolus).
Esophageal stage
The esophagus is a tubular structure running from the lower part of the UES to the lower esophageal sphincter (LES). The LES is also tensioned at rest to prevent regurgitation from the stomach. It relaxes during a swallow and allows bolus passage to the stomach. The cervical esophagus (upper one third) is mainly composed of striated muscle, but the thoracic esophagus (lower two thirds) is smooth muscle. Bolus transport in the thoracic esophagus is different from that in the pharynx because it is true peristalsis regulated by the autonomic nervous system. After the food bolus enters the esophagus, passing the UES, a peristalsis wave carries the bolus down to stomach through the LES. The peristaltic wave consists of two main parts: an initial wave of relaxation that accommodates the bolus, followed by a wave of contraction that propels it. Gravity, in upright positions, assists peristalsis.
Bolus location at swallow initiation in normal swallows
The position of the head of the bolus relative to the time of pharyngeal swallow onset is a measure of swallow elicitation. The point at which the radiographic shadow of the ramus of the mandible crosses the pharyngeal surface of the tongue is commonly used as a marker for this measurement. It was initially thought that the pharyngeal swallow was normally triggered when the bolus head passed the fauces, as observed on videofluoroscopy . When the bolus head passed the lower border of the mandible more than 1 second before the swallow initiation, it was classified as delayed swallow initiation. Delayed swallow initiation is considered an important finding because the airway is open when the bolus approaches the larynx.
Recent studies, however, have revealed that preswallow bolus entry into the pharynx also occurs in healthy individuals when drinking liquids . Furthermore, as described previously, during eating of solid food, chewed bolus is aggregated in the oropharynx or valleculae before swallowing. Bolus position at swallow initiation is now known to be variable in normal eating and swallowing. This variability is especially true when consuming a food that has both liquid and solid phases. Saitoh and colleagues demonstrated that in healthy young adults eating a food made up of soft solid and thin liquid components, the leading edge (liquid component) of the food often entered the hypopharynx before swallowing. As seen in Fig. 6 , liquid enters the hypopharynx during chewing and approaches the laryngeal aditus at a time when the larynx remains open.
The location of the bolus at swallow initiation is altered by sequential swallowing of liquid . The bolus head often reaches the valleculae before pharyngeal swallow initiation, especially when the larynx remains closed between swallows.
Coordination among eating, swallowing, and breathing
Eating, swallowing, and breathing are tightly coordinated. Swallowing is dominant to respiration in normal individuals . Breathing ceases briefly during swallowing not only because of the physical closure of the airway by elevation of the soft palate and tilting of the epiglottis but also because of neural suppression of respiration in the brainstem . When drinking a liquid bolus, swallowing usually starts during the expiratory phase of breathing. The respiratory pause continues for 0.5 to 1.5 seconds during swallowing, and respiration usually resumes with expiration . This resumption is regarded as one of the mechanisms that prevents inhalation of food remaining in the pharynx after swallowing . When performing sequential swallows while drinking from a cup, respiration can resume with inspiration .
Eating solid food also alters the respiratory rhythm. The rhythm is perturbed with onset of mastication. Respiratory cycle duration decreases during mastication, but increases with swallowing . The “exhale—swallow—exhale” temporal relationship persists during eating; however, respiratory pauses are longer, often beginning substantially before swallow onset .
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


