Anatomy
Terminology
The hand and digits are described using standard terminology (Fig. 1). They are composed of a dorsal surface, a volar or palmar surface, and radial and ulnar borders. The palm is divided into thenar, midpalm, and hypothenar areas. The thenar area contains the small muscles of the thumb and is called the thenar eminence. The hypothenar area contains the small muscles of the small finger and is called the hypothenar eminence. The digits are designated as the thumb, index, middle or long, ring, and small digits. Each finger has a proximal, middle, and distal phalanx. Each finger also has three joints: the metacarpophalangeal (MCP), the proximal interphalangeal (PIP), and the distal interphalangeal (DIP) joints. The thumb has only two phalanges (proximal and distal) and two joints (MCP and interphalangeal joints). The MCP, PIP, and DIP joints are protected from injury by stabilizing structures. Collateral ligaments protect both sides and a volar plate stabilizes the undersurface of each joint.
Hand motion also is described according to standard terminology (Fig. 2). The thumb is positioned perpendicularly to the fingers, and flexion/extension is in this plane. Abduction of the thumb can either be out of the palm (palmar abduction) or in the plane of the hand (planar or radial abduction). Thumb opposition is a combination of thumb rotation (pronation), palmar abduction, and flexion. A sagittal line through the third ray defines the center of the hand. Finger abduction/adduction is described using this reference coordinate; therefore, abduction is away from the long finger and adduction is toward it. The long finger itself is able to abduct away from this line in a radial or ulnar direction.
Integument/Fascia
The palmar and dorsal skins are distinctively different with respect to structure and function. The palmar skin is thick with fibrous septa connecting the
skin to the underlying fascia. This attachment limits motion and provides a stable platform for grasping and manipulation of objects. In contrast, the dorsal skin is loose with areolar tissue between the skin and extensor tendons. This laxity creates the dorsal subcutaneous space for lymphatic and venous drainage. This structural difference accounts for the dorsal hand swelling seen during infection even when the source is located on the palmar side of the hand.
skin to the underlying fascia. This attachment limits motion and provides a stable platform for grasping and manipulation of objects. In contrast, the dorsal skin is loose with areolar tissue between the skin and extensor tendons. This laxity creates the dorsal subcutaneous space for lymphatic and venous drainage. This structural difference accounts for the dorsal hand swelling seen during infection even when the source is located on the palmar side of the hand.
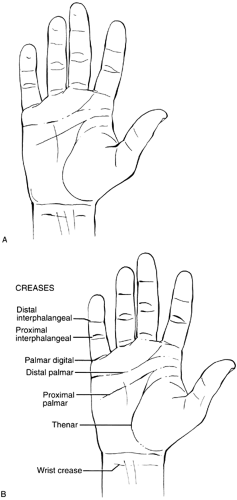 FIG. 1. A and B: Surface anatomy of the hand. |
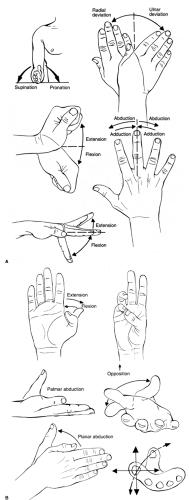 FIG. 2. A and B: Terminology for describing forearm, hand, and digital motion. |
The palmar fascia of the hand provides a stable platform for the skin and protects the underlying structures (Fig. 3). This fascia is also the insertion site for the palmaris longus tendon, allowing this muscle to flex the wrist. A septum extending from the palmar aponeurosis to the third metacarpal divides the recesses of the hand into spaces (Fig. 4). These spaces are deeper and different from the palmar surface areas described earlier. The thenar space is located to the radial side of the septum and the midpalmar space is situated on the ulnar side. These spaces can be infected primarily or secondarily following flexor tenosynovitis of the digits.
 FIG. 3. Palmar fascia of the hand provides stability and protection to the hand. |
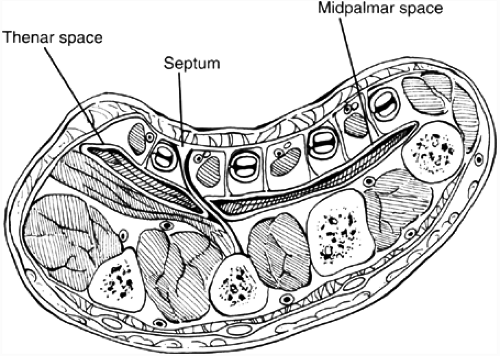 FIG. 4. Transverse section demonstrating septum from palmar fascia to third metacarpal, which divides hand into thenar and midpalmar spaces. |
Blood Supply
The radial and ulnar arteries supply the hand and digits by a series of arches (Fig. 5). The radial artery is located between the brachioradialis and flexor carpi radialis tendons at the wrist. The artery splits into two branches, with the larger dorsal branch coursing under the first dorsal compartment, through the anatomic snuffbox, between the index and thumb metacarpals, and into the recesses of the palm to form the greater part of the deep palmar arch. A smaller palmar branch travels over the flexor carpi radialis tendon, beneath or through the thenar muscles, and forms the radial component of the superficial palmar arch. The ulnar artery is located lateral to the ulnar nerve at the wrist and adjacent to the flexor carpi ulnaris tendon. The nerve and artery course into Guyon’s canal, which is bordered by the pisiform and hook of the hamate. The floor of Guyon’s canal is the transverse carpal ligament (TCL) and the roof is the volar carpal ligament (Fig. 6). The artery splits into two branches with the larger branch forming the main constituent of the superficial palmar arch. A smaller branch passes deep to connect with the radial artery and form the deep palmar arch.
A line drawn across the palm parallel to the fully abducted thumb (Kaplan’s cardinal line) approximates the location of the superficial palmar arch. This arch is located just past the distal edge of the TCL. The deep palmar arch is located one centimeter proximal to the superficial palmar arch and is beneath the flexor tendons. Although considerable variability exists, the superficial palmar arch typically provides palmar blood vessels
to the index (ulnar side), long, ring, and small fingers, whereas the deep palmar arch supplies blood vessels to the thumb and index digit (radial side) (Fig. 5). Common digital arteries originate from the superficial palmar arch and travel within the index-long, long-ring, and ring-small interspaces. These vessels divide into proper digital arteries that continue along the sides of the digits. The proper digital artery to the ulnar side of the small finger originates directly from the superficial arch. The proper digital artery to the radial side of the index finger originates from the deep palmar arch. The vascular supply to the thumb is from digital branches that originate as a common trunk (princeps pollicis artery) from the deep palmar arch. The deep arch also provides metacarpal branches that join the common digital arteries just proximal to their bifurcation into proper components.
to the index (ulnar side), long, ring, and small fingers, whereas the deep palmar arch supplies blood vessels to the thumb and index digit (radial side) (Fig. 5). Common digital arteries originate from the superficial palmar arch and travel within the index-long, long-ring, and ring-small interspaces. These vessels divide into proper digital arteries that continue along the sides of the digits. The proper digital artery to the ulnar side of the small finger originates directly from the superficial arch. The proper digital artery to the radial side of the index finger originates from the deep palmar arch. The vascular supply to the thumb is from digital branches that originate as a common trunk (princeps pollicis artery) from the deep palmar arch. The deep arch also provides metacarpal branches that join the common digital arteries just proximal to their bifurcation into proper components.
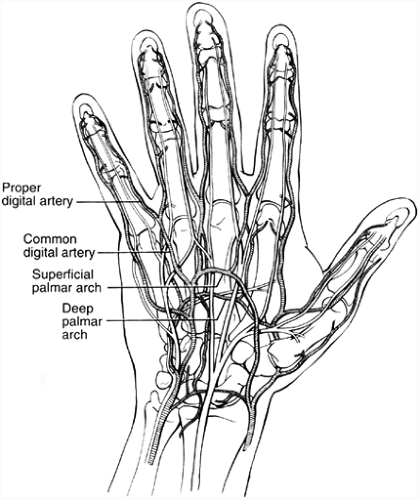 FIG. 5. Arterial blood supply to the hand. |
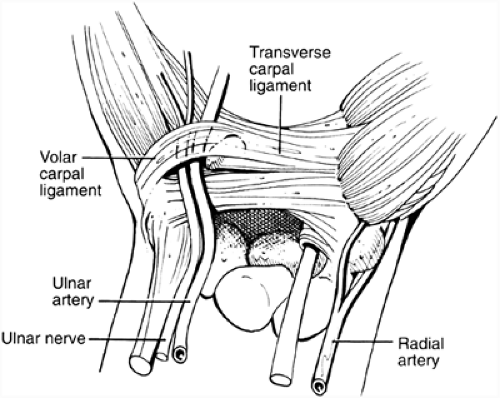 FIG. 6. The transverse carpal ligaments forms the roof to the carpal tunnel and the floor to Guyon’s canal. |
Nerves
The radial, median, and ulnar nerves supply the sensibility and motor innervation to the hand and forearm. The radial nerve enters the forearm between the two heads of the supinator muscle. The radial nerve innervates the brachioradialis and extensor carpi radialis longus, prior to dividing into the posterior interosseous and radial sensory nerves.
The posterior interosseous nerve innervates the wrist, finger, and thumb extensor muscles, whereas the radial sensory nerve travels down the forearm beneath the brachioradialis muscle adjacent to the radial artery. Subsequently, the sensory nerve passes dorsally beneath the brachioradialis at its musculotendinous junction to provide sensibility to the dorsoradial aspect of the hand and dorsum of the thumb, index, and long digits. The lateral antebrachial cutaneous nerve, which is the terminal branch of the musculocutaneous nerve, also supplies sensibility to this aspect of the hand; therefore, altered sensibility in this area can be from injury to the radial sensory and/or lateral antebrachial cutaneous nerves.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


