Running biomechanics play an important role in the development of injuries. Performing a running biomechanics analysis on injured runners can help to develop treatment strategies. This article provides a framework for a systematic video-based running biomechanics analysis plan based on the current evidence on running injuries, using 2-dimensional (2D) video and readily available tools. Fourteen measurements are proposed in this analysis plan from lateral and posterior video. Identifying simple 2D surrogates for 3D biomechanic variables of interest allows for widespread translation of best practices, and have the best opportunity to impact the highly prevalent problem of the injured runner.
Key points
- •
Running biomechanics play an important role in the development of injuries in recreationally active individuals.
- •
Performing a systematic video-based running biomechanics analysis rooted in the current evidence on running injuries can allow the clinician to develop a treatment strategy.
- •
The current literature has not risen to the level of proven injury prevention, suggesting that recommendations for modification of running form in uninjured runners would not be evidence based.
- •
When the patient presentation and physical examination findings are in agreement with abnormalities observed in a biomechanics running analysis, it serves as a potential for intervention.
Introduction
Running is an extremely common form of exercise, whether recreational or competitive. However, running injuries are also quite common. In particular, running injuries such as patellofemoral pain, iliotibial band syndrome, and stress fractures to the tibia and metatarsals have been identified as highly prevalent in runners. Although causative factors of running injuries are undoubtedly multifactorial, most agree that running biomechanics play a key role in injury development.
Numerous recent studies have identified abnormal biomechanics in persons with specific running injuries. However, the vast majority of these studies used advanced technological methods, which are expensive and uncommon in standard clinical practice. Although some variables associated with running injuries require high-tech equipment, such as instrumented treadmills and 3-dimensional (3D) motion capture systems, many of the kinematic abnormalities identified in runners with injuries can be measured using a simple 2-dimensional (2D) video-based running analysis using readily available and fairly inexpensive tools.
The objective of this article is to provide a framework for a systematic video-based running biomechanics analysis plan based on the current evidence on running injuries. Although some of the proposed variables of interest will have an impact on running performance, the primary focus of this analysis plan is to identify biomechanical factors related to common injuries in runners. Furthermore, there are many other factors that may be related or even causative for injuries while running, including training errors, current health status (ie, recent injury), and/or structural abnormalities (ie, leg length discrepancy, pes planus foot deformity etc). However, the focus of this review is restricted to running kinematics, particularly those in the sagittal and frontal plane, which may be easily viewed with standard 2D video. A running biomechanics analysis should be an integral component of the evaluation, either for the injured runner or for screening for injury prevention, to complement a physical examination and thorough history.
Introduction
Running is an extremely common form of exercise, whether recreational or competitive. However, running injuries are also quite common. In particular, running injuries such as patellofemoral pain, iliotibial band syndrome, and stress fractures to the tibia and metatarsals have been identified as highly prevalent in runners. Although causative factors of running injuries are undoubtedly multifactorial, most agree that running biomechanics play a key role in injury development.
Numerous recent studies have identified abnormal biomechanics in persons with specific running injuries. However, the vast majority of these studies used advanced technological methods, which are expensive and uncommon in standard clinical practice. Although some variables associated with running injuries require high-tech equipment, such as instrumented treadmills and 3-dimensional (3D) motion capture systems, many of the kinematic abnormalities identified in runners with injuries can be measured using a simple 2-dimensional (2D) video-based running analysis using readily available and fairly inexpensive tools.
The objective of this article is to provide a framework for a systematic video-based running biomechanics analysis plan based on the current evidence on running injuries. Although some of the proposed variables of interest will have an impact on running performance, the primary focus of this analysis plan is to identify biomechanical factors related to common injuries in runners. Furthermore, there are many other factors that may be related or even causative for injuries while running, including training errors, current health status (ie, recent injury), and/or structural abnormalities (ie, leg length discrepancy, pes planus foot deformity etc). However, the focus of this review is restricted to running kinematics, particularly those in the sagittal and frontal plane, which may be easily viewed with standard 2D video. A running biomechanics analysis should be an integral component of the evaluation, either for the injured runner or for screening for injury prevention, to complement a physical examination and thorough history.
Analysis setup
Treadmill Setup
Although some studies have identified small differences in treadmill running when compared with overground running, these differences have mostly been associated with muscle activation patterns and joint forces. In general, kinematic patterns during treadmill running are very similar to those observed during overground running. As such, performing a video-based analysis of joint kinematics while running on a treadmill should provide valuable insight into running kinematics during overground running and is more practical for performing this evaluation.
Running velocity affects lower extremity kinematics. Therefore, matching treadmill speed to a similar speed at which an injured runner experiences symptoms should be accommodated if possible. When evaluating a symptom-free runner, 1 strategy that can be used is to set the treadmill speed to match the running velocity of the runner when performing a “long run,” which is a common term used for the longest distance run in the recent past. The rationale for selecting this speed is that if runners are demonstrating abnormal biomechanics while performing longer runs, these faults will accumulate over the longer exercise period and may contribute to running injuries.
Cameras
Many high-definition cameras are available at varying price points. Both image resolution and temporal resolution should be considered when selecting cameras for video-based movement analysis. Many video cameras have excellent image resolution, but are limited to 30 frames per second. Cameras with higher frame rates (eg, ≥120 Hz) can provide cleaner images that are easier to evaluate and more appropriate for the evaluation of running kinematics. More recently released smartphones and tablets can be adjusted to acquire video at high frame rates and provide adequate video for this purpose.
Views
When performing a video-based analysis it is recommended that, at a minimum, 2 orthogonal (at right angles to each other) views are included. The analysis provided in this article uses a lateral view and a posterior view. Others may include an anterior view or lateral views from both sides. Multiple views from each camera, including zoomed-in views on the foot and ankle as well as zoomed-out views of the entire body, can be helpful. Many of these preferences will need to be modified to work within the constraints of the clinical environment. Maintaining a reproducible camera location and a fixed orthogonal angle to the treadmill is important to performing a reliable analysis. Recent studies have found the reliability of a single camera analysis to vary significantly, with some metrics showing excellent reproducibility (knee flexion, rear foot kinematics) and others demonstrating poor reproducibility (heel-to-center of mass distance). There is also evidence that experience can improve the reliability of measurements made on video-based kinematic evaluations, so it is important for the clinician to practice running evaluations regularly to improve reliability.
Markers
Application of markers for identification of anatomic landmarks can be useful when performing a video-based running analysis. These markers need not be expensive retroreflective tape-based markers. Any bright colored tape can be used for this purpose. Whenever possible, tape should be applied directly to the runner’s skin. This is imperative when performing research-level 3D motion analysis. However, adapting these methods for use in a clinical setting may require markers over clothes. In these situations, it is recommended that the runners wear tight-fitting running sportswear to minimize the movement of the markers from clothing during running. In the images presented throughout this article, the following landmarks are identified and marked: C7 spinous process, posterior superior iliac spines, anterior superior iliac spine, greater trochanter, lateral knee joint line, lateral malleolus, midpoint of the calf, superior and inferior portions of the heel shoe counter, and head of the fifth metatarsal. This is an example of a common set of anatomy landmarks that are useful to evaluate during running and can be modified to suit the needs to the evaluation.
Warmup and Analysis Plan
It is advisable to allow for a period of time for the runner to run on the treadmill at the target speed to accommodate to the environment. Studies have identified changes in kinematics deviating from normal running mechanics with treadmill running up to the initial 6 minutes. Therefore, an acclimation period of 6 to 10 minutes should be used when possible before evaluation. It is also important consider the nature of symptom provocation in an injured runner. If a runner experiences symptoms after a number of minutes or miles, it may be necessary to acquire video with the runner in a fatigued state, after a period of running and consistent with their symptom history.
When performing a movement analysis of any type, it is critical to execute the analysis systematically. We present a distal-to-proximal analysis plan. The order of the evaluation is not critical. However, it is extremely important to perform the entire evaluation, including all segments, joints, and whole body variables consistently, to avoid missing subtle yet potentially important kinematic abnormalities. Although numerous freeware options exist with extremely helpful tools for measuring biomechanical variables on running video (angles, distances, etc), it is generally not necessary. Most of the metrics in this article can be easily identified visually on slow motion video, or evaluation when progressing through the video frame by frame. To date, cutoffs for kinematics to be identified as abnormal, or predictive of injury, do not exist. As such, the analyses included here does not provide the reader with specific angles or measures that are “abnormal.” Each metric is described, and indicators of normal kinematics are provided. It is the responsibility of the evaluator to determine what threshold for normal and abnormal should be applied to an individual runner and associated with the biomechanical contributor to injury.
Phases
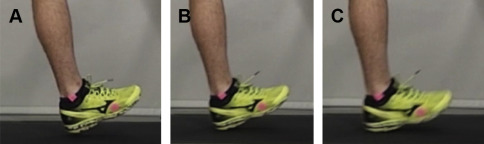
It is important to identify specific moments within the running cycle that can be used for evaluation. Many of the phases of the running cycle are clear. However, particularly for evaluating stride mechanics, it is important to differentiate between video frames of rapidly evolving events. Take, for example, the images provided in Fig. 1 . Fig. 1 A is the final frame of the swing phase, Fig. 1 B displays initial contact, and Fig. 1 C displays loading response (which is identified by the presence of shoe deformation in the image). Different kinematic variables are evaluated on images from different phases of running. It is important for the evaluator to become familiar with identifying each of these phases (and others as described elsewhere in this article). Inconsistent identification of phases of running in evaluating biomechanics of running gait will make performing a reliable analysis impossible.
Side view
Foot Strike Pattern
Identification of foot strike pattern can be easily performed on slow motion video or by evaluating video in a frame-by-frame manner ( Fig. 2 ). It is recommended to always confirm foot strike pattern in this fashion, because even after considerable practice, it is not uncommon to misidentify a foot strike type when observing running at full speed. Foot strike types can be categorized as forefoot strike (FFS), midfoot strike, and rear foot strike. Recent literature suggests that video-based identification of foot strike patterns by a single rater are highly reliable, although interrater measures was found to be less reliable. At this time, there is limited evidence that any 1 foot strike pattern is more or less likely to cause a runner to sustain an injury. However, this is an area of active research and data on this issue are emerging. One study on competitive collegiate runners suggested that runners with a rear foot strike pattern developed more repetitive overuse injuries when compared with runners with an FFS pattern. And although these finding suggest possible association between foot strike patterns and running injuries, more work is necessary before broad conclusions on foot strike recommendations can be made to modify injury risk.
Foot Inclination Angle at Initial Contact
The angle created by the sole of the shoe and the treadmill belt is noted as the inclination angle of the foot (relative to a global coordinate system, not the tibia) at initial contact ( Fig. 3 ). This variable is not applicable for midfoot strike and FFS runners.
A recent study by Wille and colleagues found inclination angle to be particularly important in estimating ground reaction forces and joint kinetics during running. Specifically, increased foot inclination angle was found to be related to higher peak knee extensor moments, increased knee energy absorbed, higher peak vertical ground reaction force, and greater braking impulse during running. Each of these variables has been implicated in injury biomechanics, suggesting that a very high foot inclination angle at initial contact may not be desirable. This may be a source for intervention in runners who experience injuries associated with high ground reaction forces or excessive joint kinetics. There are no cutoffs at which this angle is determined to be abnormal. Rather, it is likely on a sliding scale, where lower values are generally associated with lower ground reaction forces and joint kinetics, and higher values as associated with increased forces. However, it should be noted that a high foot inclination angle in isolation may be a benign finding and needs to be evaluated in the context of the entire running evaluations (see Overstriding).
Tibia Angle at Loading Response
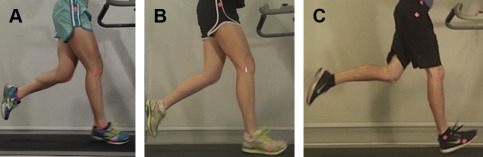
The vertical alignment of the lower leg during loading response can be a valuable indicator of stride mechanics. Video of the runner should be evaluated using freeze-frames at the moment of loading response (as the shoe begins to deform just after initial contact). The alignment of the lower leg relative to a vertical line in the video field of view can be evaluated easily. An extended tibia is identified when the lateral knee joint marker is posterior to the lateral malleolus marker ( Fig. 4 A). Conversely, a flexed tibia is identified when the lateral knee marker is anterior to the lateral malleolus ( Fig. 4 C), and when these 2 markers are directly vertical to one another, this would be identified as a vertical tibia ( Fig. 4 B). For a runner that suffers from impact-related running injuries, an extended tibia is not ideal. A vertical or flexed tibia allows the runner to dissipate impact more readily though knee flexion.
Similar to foot inclination angle, the tibia angle in itself may not be meaningful in isolation. It is a variable that can be grouped in a series of stride mechanics variables to better describe the characteristics of the runners stride and biomechanical risk profile.
Knee Flexion During Stance
Peak knee flexion angle during stance may occur at slightly different phases in different runners. It is recommended to scroll through stance phase frames to identify maximum knee flexion. Key aspects of knee flexion during stance include the peak amount of knee flexion and the knee joint excursion during stance (difference in angle from initial contact to peak knee flexion). In general, normal peak knee flexion approaches approximately 45° at midstance ( Fig. 5 ). Although explicit cutoffs have not been developed for this variable, a runner who demonstrates considerably less than 45° of knee flexion may suggest reduced shock absorption, and intervention may be warranted. Some data exist suggesting that lower knee flexion (<40°) may be associated with certain subgroups of patients with patellofemoral pain. Knee stiffness, a variable that includes both reduced knee flexion and/or increased knee flexion moment during stance phase, may be associated with tibial stress fractures.
Hip Extension During Late Stance
Reduced hip extension during late stance is a common observation in the recreational runner ( Fig. 6 ). It is traditionally believed that lack of hip extension may be associated with reduced flexibility of the iliopsoas muscle. However, the optimal amount of hip extension during running remains elusive. It is possible that the required amount of hip extension is not the same for each runner, but related to other characteristics of their running form. For example, a fairly slow runner may have a very compact stride, demonstrate approximately 10° of peak hip extension and not require any intervention. However, a different runner, with a long stride and perhaps a faster pace, may also have approximately 10° of hip extension, but also concurrently demonstrate a significant overstride pattern (landing with the foot out in front of the center of mass) with higher impact loading and braking forces. The latter runner may require stride modification or improved hip extension during running to modify these forces that could contribute to injury. Commonly observed compensations for persons with reduced hip extension include (1) increased lumbar spine extension, (2) bounding, a strategy to increase float time to increase overall stride length in the absence of adequate hip extension, (3) increased overstriding, including excessive reaching during initial contact as a strategy to increase stride length, and (4) increased cadence to increase running speed in the presence of a limited hip extension.




