Abstract
Introduction
Traumatic cauda equina syndromes due to projectile wounds often have a poor prognosis. We report on an unusual ballistic cauda equina traumatism with a good functional outcome.
Clinical case
A 44-year-old man was admitted to emergency room for an incomplete cauda equina syndrome after trying to kill himself by means of a pneumatic nail gun. The nail had gone right through the third lumbar vertebra. Because of the stability of the fracture, orthopaedic surgery was not indicated. Neurological recovery was progressive. At 6 months, there was still a partial L5–S1 motor deficit on the left side but the patient could walk without crutches, and within an unlimited walking distance.
Discussion
Initial imaging displayed a projectile trajectory focused on the spinal canal on level L3, which could have been considered as bad prognosis. The positive analytic and functional outcome correlates with the limited neurological tissue damage, probably explained by the ballistic properties of the projectile.
Conclusion
Apart from the influence of a possible surgical act, the neurological and functional prognosis of a traumatic cauda equina syndrome caused by a projectile also depends on its physical characteristics.
Résumé
Introduction
Les syndromes de la queue de cheval (SQC) secondaire à un traumatisme balistique ont généralement un pronostic fonctionnel reservé. Nous rapportons ici un cas de SQC d’étiologie balistisque atypique avec une bonne évolution fonctionnelle.
Cas clinique
Un homme de 44 ans a été admis aux urgences pour un SQC incomplet après une tentative de suicide au moyen d’une clouteuse pneumatique. Le clou a traversé la vertèbre L3. Aucune chirurgie orthopédique n’a été proposée en urgence en raison de la stabilité de la lésion rachidienne. La récupération neurologique a été progressive : à six mois, il persistait un déficit partiel à gauche, mais le patient pouvait marcher sans l’aide de béquilles sur un périmètre non limité.
Discussion
L’iconographie initiale, en nous révélant un trajet balistique centré sur le canal rachidien en L3, aurait pu nous faire envisager un mauvais pronostic. La bonne évolution analytique et fonctionnelle reflète le faible délabrement tissulaire neurologique, probablement expliqué par les caractéristiques balistiques du projectile.
Conclusion
Le pronostic neurologique et fonctionnel d’un SQC par traumatisme balistique dépend également des propriétés physiques du projectile.
1
English version
1.1
Introduction
A traumatic cauda equina syndrome due to a projectile wound is a rare clinical situation .
Epidemiologic data generally refer to spinal cord injuries, mainly due to gunshot more than stab wounds . Neurological recovery is often poor and for spinal cord injuries due to gunshot wounds, the complete nature of the initial palsy and the importance of anatomical damage would explain this poor prognosis . We report a traumatic cauda equina syndrome due to an atypical violent projectile whose final evolution is in accordance with the initial favourable criterions.
1.2
Case report
A 44-year-old patient was admitted in emergency room after an attempted suicide by means of a pneumatic nail gun. On initial clinical examination, there was a para-umbilical entry wound on the right side and an exit wound on the left lumbar side on level L3. Cauda equina syndrome was not complete: on the left side, motor deficit went from L4 to S1 nerve roots, with fibularis and tibialis anterior muscles graded 0/5 on the MRC scale, gastrocnemius , soleus and tibialis posterior muscles graded 1/5. On the right side, motor deficit only concerned the sacral nerve roots. Clinical examination of cutaneous sensitivity highlighted saddle hypoesthesia and a complete loss of sensitivity in the left L2 dermatome. Cutaneous plantar reflexes were indifferent. On genito-urinary aspects, there was a hypotonic anal sphincter graded 2/5, and cutaneous anal and bulbocavernosus reflexes were abolished. The patient did not receive any perfusion of corticoids since the acute peritonitis required a digestive surgery in emergency.
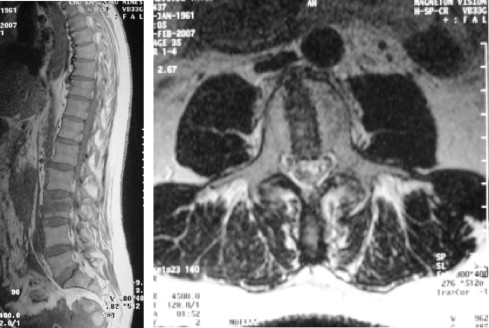
The lumbar CT scan and MRI showed the nail trajectory going through the third lumbar vertebra and the spinal canal. There was no evidence of a compressive intraspinal or retroperitoneal haematoma ( Figs. 1 and 2 ).

After 1 month in intensive care unit, the patient was transferred to Physical Medicine and Rehabilitation Department. On clinical examination, an asymmetrical cauda equina syndrome, predominant on the left side, persisted with a motor deficit going from L4 to S5 territories (extensor hallucis , extensor digitaris longus , tibialis anterior, fibularis graded 0/5, gastrocnemius , soleus , tibialis posterior graded 1/5, gluteus medius graded 3/5, quadriceps femoris and ilio-psoas 5/5), an hypotonic anal sphincter with a weak voluntary contraction, hypoesthesia with hyperpathia from S1 to S3 dermatomes on the left side and abolished bulbocavernosus reflexes. Transfers supine to sit and bed to chair were done. Gait on a few steps was possible with two people helping, but quickly impaired by orthostatic hypotension.
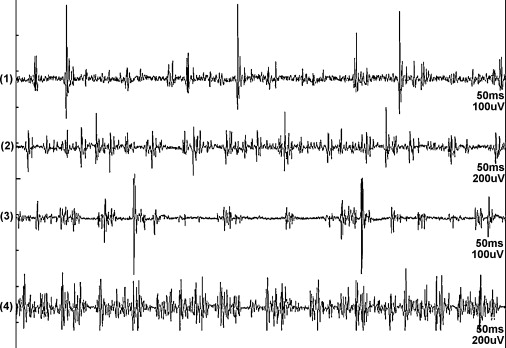
The perineal electroneuromyography showed a prolonged bulbocavernosus reflex latency up to 58 ms on the right side and 50 ms on the left one (normal value less than 44 ms for the laboratory), and denervation activity on bilateral S3 to S5 myotomes associated with reinnervation potentials. ( Fig. 3 ). In the left lower limb, denervation activity could be seen in L5 and S1 myotomes, associated with reinnervation potentials.
Rehabilitation care consisted in progressive vertical positioning, reinforcement of the paretic muscles, control of postural balance and gait. Neuropathic pain was treated by adequate antalgic drugs and transcutaneous electrical nerve stimulation.
By the end of hospitalisation, the patient could walk with a steppage gait, a loss of step propulsion and an ankle instability. An Aircast ® orthesis was the only one accepted by the patient.
At 6 months, a partial motor recovery was noted ( tibialis anterior, extensor hallucis , extensor digitaris longus and triceps suralis graded 2/5). Clinical examination of cutaneous sensitivity and genito-sphincter functions was back to normal and neuropathic pain went away.
Gait was stable on a flat surface, without walking assist device, but with a minor steppage.
Walking distance was unlimited. The patient refused a drop foot orthosis, including a simple elastic one.
1.3
Discussion
We have few epidemiologic data on cauda equina-penetrating traumatisms but they seem to be mainly due to gunshot and stab wounds .
If such reports of atypical clinical cases of cauda equina traumatisms have been made , this one focuses on an atypical ballistic cause, which has never been described before to our knowledge.
During the acute phase of a cauda equina ballistic wound, what is difficult for clinicians is to predict the functional prognosis of the patient. By analogy, with spinal cord injuries at the same level, analytic and functional recovery is poor .
Established good prognostic factors are the respect of motor command, the low severity of the initial motor deficit and of its extent and the small importance of the locoregional tissular damage.
Undergoing decompression surgery or even intraspinal fragments removal and the delay to surgery are discussed prognostic factors .
This case history presents initial clinical features of relatively good prognosis, with a limited impairment (L4 to S5 roots on the left side and S2 to S5 roots on the right) and an incomplete neurological lesion. Iconography suggested though an important tissular damage, with a projectile trajectory going through the whole spinal canal. Analytic and functional recovery was of good quality, which goes against the impression given by the iconography. The good genito-urinary recovery is also atypical in these cauda equina traumatisms .
During a ballistic trauma, the extent of tissular damage is related to kinetic energy transferred from the projectile to the tissues. This energy transfer is increased by several factors, such as trajectory (tilt or rotation after impact), fragmentation or deformation of the projectile . There are two types of tissular damages: the permanent cavity or crushing, corresponding to definitely destroyed tissues and the temporary cavity, or stretching, corresponding to a short stretching while the projectile passes through the tissues. Consequences of stretching on tissue’s viability is variable .
In this case report, cauda equina syndrome was due to a nail, which went through the abdomen and the lumbar spine. Kinetic energy provided by a nail gun is comparable to the one of a conventional firearm, since muzzle velocity can reach 100 to 150 m/s (330 to 490 ft/s).
By way of contrast, the ballistic properties of the nail are very different. The nail is a small calibre projectile, which must be stiff enough to pass through a woodcut without changing trajectory or fragmenting. Thus, the permanent tissular cavity has a small diameter and the temporary one is of limited importance. This could explain the limited tissular damage in our case and partially the good analytic and functional prognosis.
1.4
Conclusion
The functional prognosis of cauda equina syndromes due to a ballistic traumatism not only depends on the initial extent of lesions or the possibility of a surgical act but also on the properties of the projectile. Most of cauda equina syndromes are due to firearms. In case of an atypical projectile, the prognosis may be better.
2
Version française
2.1
Introduction
Un syndrome de la queue de cheval (SQC) traumatique provoqué par un projectile est une situation clinique rare . Les données épidémiologiques concernent le plus souvent des lésions médullaires majoritairement dues à des armes à feu, devant les plaies par armes blanches . La récupération neurologique est souvent mauvaise et dans le cas des lésions médullaires par arme à feu, il semblerait que le caractère complet du déficit initial et l’importance du délabrement anatomique explique ce mauvais pronostic . Nous rapportons le cas d’un SQC causé par un traumatisme violent et atypique dont l’évolution est conforme aux critères initialement favorables.
2.2
Cas clinique
Un patient de 44 ans est admis aux urgences après une tentative de suicide avec une clouteuse pneumatique. L’examen clinique initial décrit un orifice d’entrée paraombilical droit et un orifice de sortie paralombaire gauche de niveau L3. Le SQC est incomplet : à gauche le déficit moteur s’étend des racines L4 à S1 avec les muscles fibularis et tibialis anterior cotés 0/5 sur l’échelle MRC, gastrocnemius , soleus et tibialis posterior cotés à 1/5. À droite, le déficit moteur ne concerne que les racines sacrées. Sur le plan sensitif, il existe une hypoesthésie en selle, ainsi qu’un déficit S2 complet du coté gauche. Les réflexes cutanés plantaires étaient indifférents. Sur le plan vésicosphinctérien, on notait une hypotonie du sphincter anal avec un testing à 2/5, des réflexes cutanés anaux et bulbocaverneux abolis. Le patient n’a pas reçu de traitement par corticothérapie intraveineuse en raison d’une péritonite nécessitant une chirurgie digestive en urgence. Une tomodensitométrie et une IRM lombaire mettaient en évidence le passage transcorporéal L3 du clou traversant totalement le canal rachidien et l’absence d’hématome compressif intracanalaire ou rétropéritonéal ( Fig. 1 et 2 ).

Related posts:
 Proposition pour un enseignement international de MPR en anglais, coordonné par le Cofemer avec la participation des grandes associations nationales de MPR françaises (Cofemer, Sofmer, Syfmer et Fedmer) et des Annals of PRM
Proposition pour un enseignement international de MPR en anglais, coordonné par le Cofemer avec la participation des grandes associations nationales de MPR françaises (Cofemer, Sofmer, Syfmer et Fedmer) et des Annals of PRM
 Translation and French cultural adaptation of a decision making tool for patients orientation after total hip or knee arthroplasty
Comparison of the repercussions of cLBP in four French-speaking countries
Drug treatments for spasticity
Agenda
Translation and French cultural adaptation of a decision making tool for patients orientation after total hip or knee arthroplasty
Comparison of the repercussions of cLBP in four French-speaking countries
Drug treatments for spasticity
Agenda
 Effectiveness of nitrous oxide and analgesic cream (lidocaine and prilocaine) for prevention of pain during intramuscular botulinum toxin injections in children
Effectiveness of nitrous oxide and analgesic cream (lidocaine and prilocaine) for prevention of pain during intramuscular botulinum toxin injections in children
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


