Aftercare of the Injured and Operated Hand
General Information
Appropriate aftercare is critical to a successful result following hand injuries or elective hand surgery. Following injury or operation, specific splints or casts are necessary in most situations. Rehabilitation protocols administered by a certified hand therapist are paramount to the recovery of patients with hand injuries or for patients recovering from hand surgery. Disregard for the principles of hand immobilization and hand rehabilitation is one of the single greatest contributing factors to poor outcome from hand surgery or injury. In general, hand surgery is a discipline that frequently employs motion. Treatment of hand conditions has as its primary goal early motion. Dressing, splints, and rehabilitation protocols should facilitate this goal.
Wound Dressing and Edema Control
Postoperative dressings for the hand and wrist should be nonadherent and nonconstrictive. A moist wound covering such as Adaptic or Zeroform should be applied to the wound, followed by dry gauze sponges. A forgiving circular dressing such as soft-roll or Webril is used to stabilize the sponges. The preferred outer wrap is stockinet cut on the bias. Alternatively “ace-wraps” can be used as a hand and arm dressing but care must be exercised during application because of a tendency by many to stretch this elastic bandage too tightly, causing a constrictive dressing. If a digital dressing is to be applied, a small 2 × 2 inch gauze applied with a lightly applied, single-layer 2-in. Kling, secured with a top dressing of 1/2-in. Coban may be used. If motion is to be encouraged after the application of hand, wrist, or digital dressing, the dressing should not be thick and multilayered but lightly applied particularly about the joint creases. Sustained hand elevation with application of ice is encouraged to decrease postoperative or postinjury edema. This can be facilitated by using commercially available arm elevators or by propping the extremity above the heart using pillows (Fig. 1).
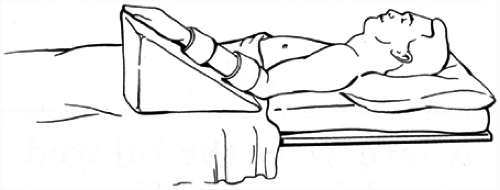 FIG. 1. Arm elevation. |
Hand Position
The safe position of immobilization of the proximal interphalangeal joint (PIP) is approximately 30 degrees of flexion, because this puts the collateral ligaments of the PIP joint on their greatest tension. Theoretically, therefore, the ligaments should not be subject to contracture following a period of immobilization and prolonged PIP stiffness should not result. Similarly, the metacarpophalangeal (MCP) joint is protected from contracture when it is immobilized in 90 degrees of flexion. This places the collateral ligaments on maximum tension because of the “cam effect” of the MCP. The shape of the metacarpal head is oval such that, when the MCP is held in extension, the collateral ligaments are lax, and they are taught when the MCP is held in maximum flexion (Fig. 2). Immobilizing the MCP in maximum flexion prohibits postsplinting
stiffness of the MCP. The “prehensile position of the wrist” or the position of function of the wrist is approximately 15 degrees of extension. Prolonged positioning of the wrist in flexion promotes stiffness of the digits by promoting contracture of the intrinsic musculature. The wrist has a wide range of motion in flexion and extension and it is more desirable to sacrifice wrist flexion than wrist extension because most hand activities depend on wrist extension. As a general rule for immobilization in the upper extremity, joints above and below the area in question should be immobilized.
stiffness of the MCP. The “prehensile position of the wrist” or the position of function of the wrist is approximately 15 degrees of extension. Prolonged positioning of the wrist in flexion promotes stiffness of the digits by promoting contracture of the intrinsic musculature. The wrist has a wide range of motion in flexion and extension and it is more desirable to sacrifice wrist flexion than wrist extension because most hand activities depend on wrist extension. As a general rule for immobilization in the upper extremity, joints above and below the area in question should be immobilized.
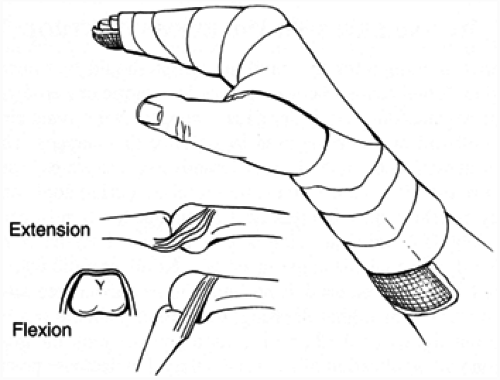 FIG. 2. Safe position. Inset shows tension applied to the collateral ligaments with the MCP joint in the “safe position.” |
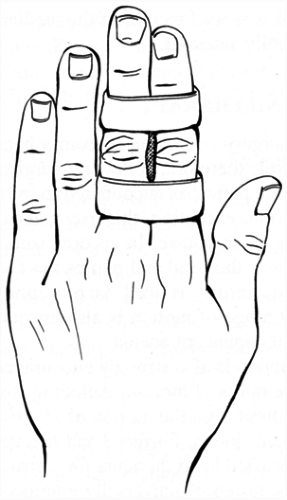 FIG. 3. Buddy taping.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|




