Acute Patellar and Chronic Patellar Instability
Eric J. Wall
Jay C. Albright
Sarah R. Steward
DEFINITION
Patellar instability in children and adolescents usually involves an episode of complete dislocation of the patella from the trochlear groove. Occasionally, there can be episodes of patellar subluxation without gross dislocation.
There are two main types of patellar dislocation:
Acute traumatic patellar dislocation in athletic, nonlax individuals
Atraumatic dislocations or subluxation secondary to ligamentous laxity
Children between the ages of 10 and 17 years have the highest risk for traumatic and atraumatic patellar dislocation.12 The incidence of primary patellar dislocation in this age group is reported at 29 per 100,000 annually and is more common in females.9
Acute traumatic patellar dislocation is frequently (28% to 39%) associated with articular surface fractures of the patella or of the lateral femoral condyle.3, 22
Most traumatic patellar dislocations tear the medial patellofemoral ligament (MPFL), which is the primary restraint to patellar dislocation. This may lead to persistent apprehension or recurrent instability of the patellofemoral joint.
Nonoperative treatment is indicated for patellar dislocation associated with ligamentous laxity and for first-time traumatic patellar dislocation that is not associated with a repairable articular surface injury.
Care must be taken to avoid realignment surgery for patients with patellofemoral pain and no clear evidence of instability.
ANATOMY
The medial restraints of the patellofemoral joint are made up predominantly of the medial retinaculum and the MPFL. Forty percent to 60% of the resistance to lateral translation is supplied by the MPFL.19 The MPFL provides 50% to 80% of the restraining force to lateral patellar displacement.13
Traumatic dislocation of the patella occurs almost exclusively in the lateral direction and often results in a tear of the MPFL at its femur insertion, patellar origin, or in its midsubstance (FIG 1A). The MPFL can tear in multiple sites during a single dislocation.
The MPFL is a flat band adjacent to the medial retinaculum that is about 15 mm wide. It extends from the superomedial aspect of the patella, about 10 to 15 mm distal to the superior pole, to the medial epicondylar area, just above and posterior to the origin of the medial collateral ligament, and distal to the adductor tubercle25 (FIG 1B).
During limited-incision surgical approaches, anatomic landmarks are not reliably identified due to small incisions. Fluoroscopy and isometry is needed to confirm the proper site of MPFL reattachment location (see TECH FIG 1A,B).
Although there is some controversy, most believe that the native MPFL arises from the femur just distal to the growth plate near the medial epicondyle in a skeletally immature patient.12, 16, 20, 32
The common finding of a lateral femoral condyle bone bruise at the sulcus terminalis suggests that dislocation usually occurs at 70 to 80 degrees of flexion.29
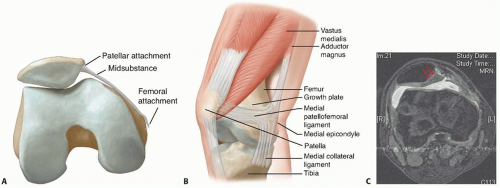
FIG 1 • A. The MPFL can tear at its patellar origin, its femoral origin, or in its midsubstance. B. The MPFL tethers the medial patella to the medial condyle of the femur. It arises from the superior two-thirds of the medial border of the patella and inserts between the adductor tubercle and medial epicondyle. Its insertion is just distal to the growth plate. C. The entire medial cartilaginous facet of the patella has separated from the underlying bone after a primary traumatic patellar dislocation. (continued)
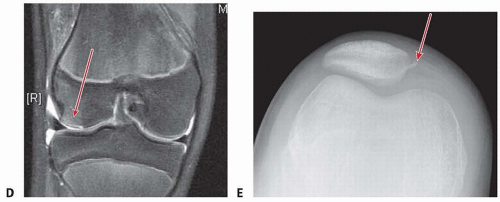
FIG 1 • (continued) D. After patellar dislocation, this patient has an osteochondral fracture of the lateral femoral condyle (arrow). E. Insignificant avulsion fracture off medial patella (arrow), which is pathognomonic for patellar dislocation.
Traumatic dislocation can cause a serious fracture of the medial patellar facet (FIG 1C) or the lateral femoral condyle (FIG 1D) and can be cartilaginous or osteocartilaginous.
Stanitski and Paletta33 found a 71% incidence of osteochondral injury at arthroscopy after patellar dislocation, most of which was radiographically occult.
More frequently, there is a less serious nonarticular avulsion fracture of the MPFL off the medial patella. There can be an immediate or delayed appearance of an ossific lesion, which rarely needs removal or reattachment, at the avulsion site off the medial patella (FIG 1E).
PATHOGENESIS
Noncontact patellar dislocation during sports usually involves lower extremity internal rotation combined with knee valgus on a planted foot (a mechanism very similar to anterior cruciate ligament injury).
Less commonly, patellar dislocation is caused by a direct blow on a valgus bent knee that pushes the kneecap laterally.
The bony anatomy of the patellofemoral joint may be abnormal with a deficient lateral femoral slope of the trochlear groove, a shallow trochlear groove, patella alta, patellar tilt, or a lateralized and/or hypoplastic tibial tubercle. These factors can increase the risk of dislocation by decreasing the force needed to laterally translate or dislocate the patella.7
The lateral retinaculum may also be tight, characterized by less than 12 mm of medial translation.15
The alignment of the lower extremities must also be considered. The quadriceps angle may be greater than average, increasing the lateral translational force.
So-called miserable malalignment syndrome may exist, including excessive femoral anteversion with or without increased external tibial torsion.14, 15
Multiple anatomic factors are theorized to increase the risk of patellar dislocation, such as family history, increased Q angle, femoral intorsion, tibial extorsion, knee valgus, trochlear groove dysplasia, and foot pronation. Only patella alta is a proven risk factor.2 MPFL reconstruction results are not diminished by patella alta or tibial tuberosity-trochlear groove (TT-TG) distances of up to 25 mm.21
NATURAL HISTORY
Patients with an atraumatic presentation of instability or dislocation of the patellofemoral joint have a higher likelihood of repeat instability episodes, despite aggressive physical therapy and bracing.14, 15
A recent study on adolescents with traumatic first-time patellar dislocation reports a 70% recurrence rate.28
Young age was also associated with recurrence, as was a positive family history.9
At 6 months after patellar dislocation, only 69% of patients had returned to sports.2
At 2 to 5 years of follow-up after patellar dislocation, Fithian and coworkers9 showed no radiographic or scintigraphic evidence of degenerative joint disease.
At 6 to 26 years of follow-up after nonoperative treatment for patellar dislocation, 22% of knees showed arthritic changes, compared to 11% of each patient’s opposite uninjured knee.17
At least 30% to 50% of patients with patellar dislocation will have knee pain more than 2 years after injury, and 69% of athletes will decrease their sports activity.11
Young age and skeletal immaturity, especially in females, is associated with worse prognosis.23
Patellar dislocation, especially recurrent patellar dislocation, is associated with patellofemoral arthritis in adulthood.34
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients with an acute traumatic patellar dislocation often present to the emergency room with a history of a noncontact or contact injury to their knee. Many do not recognize the injury as a patellar dislocation.
An effusion is usually present after traumatic dislocation but is rarely present after atraumatic dislocations.
Like an anterior cruciate ligament injury, it is common to hear or feel a “pop” at the time of injury. If the patella completely dislocates, the athlete may be found to have a deformity of the knee and may be unable to actively extend the knee.
Most episodes of patellar dislocation spontaneously reduce in the field.
If the patella is still dislocated, the emergency physician usually performs a reduction by slowly extending the knee from its flexed position.
Patellar dislocation that spontaneously reduces in the field may mimic the history and presentation of an anterior cruciate ligament tear.
A thorough examination will include the following:
Examination for effusion
Patellar glide (Patellar stability) test: With the knee flexed 25 to 30 degrees, the patella is gently translated laterally and compared to the opposite knee, which show less
translation. An intact MPFL will usually have a solid end point near the limit of lateral translation. Unfortunately, the patellar stability examination is often unreliable in the awake patient due to extreme apprehension to lateral translation. In this case, an examination under anesthesia can help confirm the diagnosis when the history and magnetic resonance imaging (MRI) are unclear.
Patella apprehension sign: With the knee flexed over a bolster at 25 degrees, the patella is translated laterally. If the patient exhibits apprehension, the test is positive. This is the best test for patellar instability.
J sign: Observe and palpate the patella for lateral subluxation during active range of motion. A positive sign occurs when the patella pulls laterally as the knee reaches full extension, tracing the path of an upside-down “J.” This can identify proximal alignment issues.
Femoral rotation: Average rotation is external rotation greater than or equal to internal motion.
Tibial alignment: Average axis is 10 to 15 degrees of external tibial torsion.
Patients with obvious genu valgum should have a standing alignment film with their patellas pointing forward. A plumb line drawn between the femoral head center and the center of ankle tibial plafond that passes lateral to the notch may be an indication for a guided growth hemiepiphysiodesis.
Assess for generalized hypermobility using the Beighton hypermobility score, which ranges from 0 to 9. One point accrues for each elbow that hyperextends greater than 10 degrees, each little finger that shows greater than 90 degrees extension across the metacarpophalangeal (MCP) joint, each thumb that can touch the volar forearm, each knee that hyperextends greater than 10 degrees, and one point if the patient can bend forward and touch their palms flat on the floor.
Beighton scores of four or greater may indicate generalized hypermobility.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Knee radiographs should include the anteroposterior (AP), lateral, and sunrise (or Merchant) views.
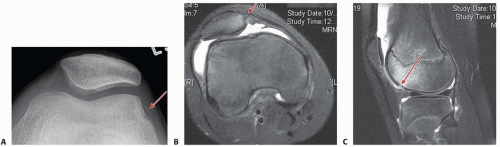
FIG 2 • A. Osteochondral fragment. Postpatellar dislocation radiographic sunrise view shows a subtle sliver of bone (arrow), which on arthroscopy proved to be a large osteochondral fracture from the lateral condyle that was repaired with screw fixation. B. MPFL tear off from the patella. MRI shows disruption of MPFL off its origin from the patella (arrow), with increased signal on medial patella. C. Lateral femoral condyle bone bruise on MRI scan after a patellar dislocation. There is a subtle break in the articular cartilage (arrow). The location of the bruise provides evidence that the patella usually dislocates with the knee in 70 to 80 degrees of flexion.
The sunrise or Merchant view requires a patient to flex the knee 30 to 45 degrees, which may be impossible owing to pain at the initial time of presentation in the emergency department. The sunrise view can usually be obtained at the first follow-up visit.
Each radiograph is evaluated for fracture or loose fragment necessitating more emergent surgical indications.
Plain radiographs can miss 40% of arthroscopically documented chondral or osteochondral lesions. Many reparable osteochondral injuries show only a sliver of bone on one view in the plain radiographic series, which can be easily overlooked (FIG 2A).
Because of the high rate of occult articular or osteoarticular injury, we recommend an MRI scan on patients who present with a large traumatic effusion after patellar dislocation.
The site of MPFL ligament disruption can often be identified on MRI. MRI is reported to be 85% sensitive and 70% accurate30 (FIG 2B). The MPFL is torn or stretched at multiple sites after a patellar dislocation episode in 27% to 46% of cases.8, 16
MRI after acute traumatic patellar dislocation shows a signature bone contusion pattern (FIG 2C). There was a 100% occurrence of anterior third of the lateral femoral condyle bone bruises and 96% occurrence of medial patellar bone bruises in one study.27 This bone bruise pattern is distinct from that associated with anterior cruciate ligament tears.
DIFFERENTIAL DIAGNOSIS
Anterior cruciate, medial collateral, lateral collateral, or posterior cruciate ligament tear
Meniscal tear
Knee contusion
Osteochondral injury
Sinding-Larsen-Johansson disease
Patellofemoral pain syndrome
NONOPERATIVE MANAGEMENT
Some 17% to 70% of adolescent patients will suffer a recurrent patellar dislocation after nonoperative management of their first patellar dislocation.9, 28Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








