Abstract
Objective
This study was designed to compare the effects of different ankle taping methods on lower leg EMG and subtalar kinematics.
Methods
Twelve healthy volunteers were tested on an inversion platform in one of three taping conditions: non-elastic basketweave, elastic adhesive bandage wrap and non-taped control. Muscle activation and range of motion data were collected during an inversion of 35 degrees using a Biometrics ® datalogger. Testing was done before and after 30 minutes of treadmill running.
Results
Significant differences were noted in total inversion, time to peak inversion and rate of inversion. While total inversion did not differ between tape conditions, the rate of inversion in the non-elastic condition was lower than the elastic adhesive condition, which was lower than the control. There was no effect of ankle taping style on latency of the peroneus longus .
Conclusions
The choice of ankle taping style can have significant effects on ankle biomechanics and the use of non-elastic tape reduces the rate of inversion. While the rate increased after 30 minutes of running, it was still lower than the other conditions.
Résumé
Objectif
Cette étude fut mise en place pour comparer les effets de différentes méthodes de taping de la cheville sur l’activité EMG de la jambe ainsi que sur la cinématique sous-talienne.
Méthodes
Douze volontaires en bonne santé physique furent testés sur une plateforme à inversion suivant une des trois conditions de taping : un bandage tissé non élastique, un bandage adhésif élastique et un groupe témoin sans bandage. L’activité musculaire et la gamme de mouvement ont été collectées durant une inversion de 35 degrés en utilisant un enregistreur de données Biometrics ® . Les tests furent réalisés avant et après 30 minutes de course sur tapis roulant.
Résultats
Des différences significatives ont été notées au niveau de l’inversion totale, du temps pour atteindre le pic d’inversion et du taux d’inversion. Alors que l’inversion totale ne différait pas entre les différentes conditions de taping, le taux d’inversion en condition non élastique était inférieur à celui en condition adhésive élastique, qui était lui-même inférieur à celui du groupe témoin. Il n’y a pas eu d’effet du style de bandage sur le temps de latence du muscle long fibulaire.
Conclusion
Le choix du style de taping de la cheville peut avoir des effets significatifs sur la biomécanique de la cheville et l’utilisation de bande non élastique réduit le taux d’inversion. Alors que le taux augmentait après 30 minutes de course, il continuait de rester inférieur aux autres conditions. Par conséquent, le taping peut être un complément utile au support de la cheville, limitant l’inversion au cours d’un programme de réhabilitation.
1
English version
1.1
Introduction
There is abundant literature to indicate that the ankle is one of the most commonly injured structure in the body and results in significant time-loss to participation . In sports, ankle injuries account for 15% of all reported injuries , while a lateral ankle sprain has been reported to make up 83.4% of all ankle injuries .
With the epidemiological evidence regarding ankle sprains, it has been common practice to tape the ankle to prevent injury. As a prophylactic measure, ankle taping has resulted in a reduction in either the incidence or severity of ankle sprains although one report stated that there was no change in the incidence of sprains . There is also debate in the literature about the effectiveness of ankle taping with regard to the duration of support offered. Some studies have reported that taping support is significantly reduced following exercise while others have found that taping still retains significant restriction . Perhaps the main reason that taping is used so often is that it can accommodate individual requirements such as demands of the sport, body shape, and severity of the injury . Ankle taping is thought to reduce the risk of injury, or the severity, by providing additional limitation to the ranges of motion that may overload connective tissues, for example by reducing the absolute inversion or the rate of ankle inversion .
It is likely that restriction of the range of motion (ROM) is not the only mechanism for avoiding ankle sprains. The primary function of the peroneus longus muscle is eversion and thus may play an important role in the prevention of ankle sprains. When an inversion movement is applied to the foot, the peroneus longus plays an important role as the primary defense mechanism . With regard to muscle activity and external ankle support, the data has been mixed. While some papers have indicated a detrimental effect of prophylactic ankle support on muscle activity , other publications have indicated no significant effect on muscle activity .
Many different taping techniques exist and these vary across sports and regions. It has been stated that appropriate and effective ankle taping is both an art and a science . There are certainly times when styles of taping can be outdated or not rooted in science, as was shown by Yamamoto et al. who stated that newer methods of ankle taping can offer greater support and protection compared to traditional methods . The most common type of tape used is non-elastic (NE) zinc-oxide tape and uses stirrups, horseshoes, figure-of-eight wraps and heel locks. Care must be taken when non-elastic tape is used, especially when the technique involves applying the tape circumferentially around a limb. If the tape is applied too tightly, the risk of impeding blood flow is increased and this could lead to tissue damage and even tissue necrosis. At best, comfort and performance could be detrimentally affected by taping that is too restrictive.
To avoid these potential problems, an alternative taping technique using elastic adhesive bandaging (EAB) has been developed. This alternative technique involves the use of three zinc-oxide stirrups for primary restriction, followed by figure-of-eight wraps using EAB. The theory is that the EAB not only provides adequate support but also allows functional movement without restricting blood flow to and from the tissues distal to the taping.
Unfortunately, there is a lack of research regarding the kinematic, kinetic and functional effects of different taping styles. The purpose of this study, therefore, is to answer a fundamental question: is there any difference between EAB taping and NE taping in the rate of ankle inversion or peroneal longus latency, both before and after exercise?
1.2
Methods
Twelve participants volunteered to take part in this study. All participants were free from lower extremity pathology and were in general good physical condition. All subjects were instructed in the data collection procedures, and then signed an informed consent, as approved by the local ethics board. The physical characteristics for the participants were age of 24.1 ± 6.8 years; a height of 174.2 ± 10.1 cm; and body mass of 76.7 ± 19.9 kg.
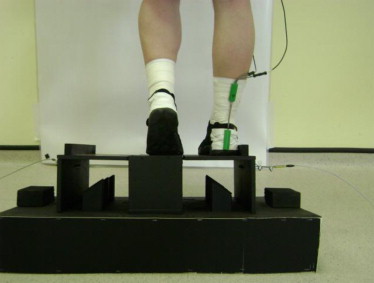
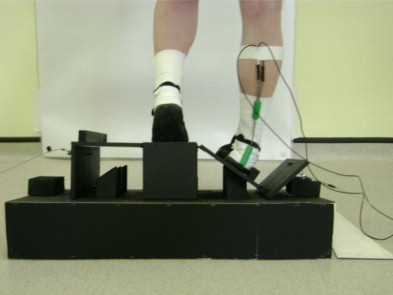
Subjects were randomly assigned to one of three test conditions: control, EAB taping, and NE taping ( Figs. 1 and 2 ). Each subject was tested in all three conditions, using a Latin Square design to counterbalance the testing sequences. The NE taping procedure used in this study was identical to that described by Perrin and outlined in Table 1 . For inversion testing, we provided a standard sports shoe to the subjects, in order to eliminate the variability of footwear in the test results.


| EAB | NE (using entirely 3.8 cm zinc oxide) |
|---|---|
| 1. Adhesive spray | 1. Adhesive spray |
| 2. Pre-wrap | 2. Pre-wrap |
| 3. 2.5 cm zinc oxide anchors | 3. Anchors |
| 4. Stirrups, start and finish medially 2.5 cm zinc oxide ( Fig. 2 ) | 4. Three stirrups, starting medially and finishing laterally |
| 5. Figure-of-8 | 5. Figure-of-8 |
| 6. Close, continuous, with 7.5 cm elastic adhesive bandage | 6. Heel locks–2 each, medial and lateral ( Fig. 3 ) |
| 7. Close, non-continuous |
Kinematic data were collected using an electrogoniometer (Biometrics Ltd, Gwent, Wales) in a procedure that had previously been validated . The electrogoniometer’s sensors were fixed with double-sided tape to the heel of the shoe and the proximal calcaneal tendon. An extra strip of 2.5 cm non-stretch tape was placed over the electrogoniometers to ensure their continued adhesion to the subject during testing. The positions of the electrogoniometer’s sensors were marked for accurate replacement after exercise and on subsequent testing days. Data were collected at 1000 Hz using a Biometrics ® datalogger equipped with an electrogoniometer and preamplified EMG electrode.
EMG data were analyzed using Acqknowledge Software (software version 3.8.3, Biopac Systems Inc., Goleta, California, USA). The raw data were bandpass filtered from 10 to 350 Hz prior to full wave rectification. The bandpass filtering values were chosen after a Fast Fourier Transformation of pilot data revealed that the bulk of the signal was contained between these points. A notch filter of 50 Hz was used to suppress electrical noise from the other equipment in the lab. The muscle activity was analyzed for time of muscle onset relative to the start of movement. The onset of muscle activity was determined by the electrical signal rising more than 2 standard deviations above the mean baseline level and remaining at that level for 30 ms. Peroneus longus latency times were determined by the time between the onset of the inversion platform movement, as recorded by the electrogoniometer, and the onset of the motor response. We determined muscle onset as being 2 standard deviations (SD) above the mean baseline EMG. The mean baseline measure was averaged from the 50 ms prior to the beginning of the inversion platform movement .
In order to test the effects in a simulated inversion, a platform was constructed based on the previously published designs . The platform permitted an unexpected inversion, but was limited to 35 degrees, as this is within the normal limits of subtalar inversion ROM . The subject placed their dominant leg on the corresponding trap door, placing their foot 2.5 cm from the raised edge of the trap door. We instructed the subject to place all their weight on the dominant stance limb and use only the toes of the contralateral limb to maintain balance ( Fig. 3 ). The subjects stood on the inversion platform facing away from the testers and the release was triggered at random intervals to lessen any possible anticipation ( Fig. 4 ). Five trials were carried out for each subject and then the subject completed 30 minutes of exercise on a treadmill wearing their own footwear. After the exercise, we tested the subjects again on the inversion platform following the same protocol as pre-exercise testing. A Grubbs test was used to test for any outliers in the data prior to statistical analysis. The means of the five trials in each condition (taping style and pre/post-exercise) for each subject were used for the repeated-measures Anova.
1.3
Results
1.3.1
Range of motion
Although the platform had a limit of 35 degrees of inversion, we noted differences in total ROM following the inversion. Both EAB and NE were significantly different from the untaped, control condition but there was no difference in the range of motion when compared between NE and EAB, either before or after exercise.
The time to peak inversion, as measured in milliseconds, showed some differences between groups. The NE condition was significantly different from either EAB or control ( P < .05) yet there was no difference between the control or EAB with respect to time to peak inversion. There were slight yet non-significant ( P = .09) changes in this variable when compared between pre-exercise and post-exercise conditions.
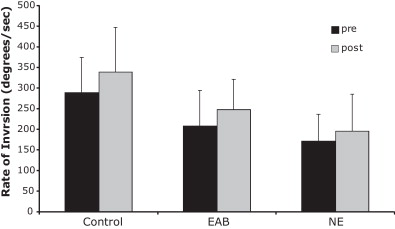
Concerning the rate of inversion (ROI), a repeated-measures Anova indicated that there was a significant difference between tape conditions ( P < .01) as well as between pre- and post-exercise ( P < .01). As the values in Table 2 indicate, the ROI for control was significantly greater than EAB, which in turn was significantly greater than NE. This was observed both pre-exercise and in the post-exercise testing. There was no interaction between tape condition and pre-/post-testing with regard to the ROI.
| Control | EAB | Non-elastic | |
|---|---|---|---|
| Total inversion (°) | |||
| Pre-exercise | 30 ± 10 | 24 ± 86 | 24 ± 6 |
| Post-exercise | 33 ± 7 a | 26 ± 5 | 24 ± 7 |
| Time: peak inversion (ms) | |||
| Pre-exercise | 112 ± 45 d | 125 ± 43 b , d | 153 ± 57 b |
| Post-exercise | 102 ± 29 d | 114 ± 37 b , d | 146 ± 68 b |
| Rate of inversion (°/s) | |||
| Pre-exercise | 289 ± 85 a | 209 ± 85 b , d | 172 ± 64 b |
| Post-exercise | 339 ± 109 a , c | 248 ± 73 b , c , d | 196 ± 89 b , c |
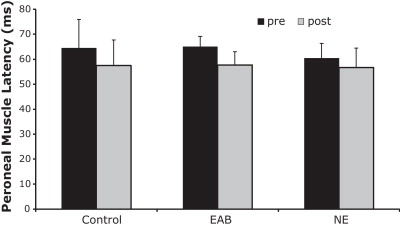
| EMG latency (ms) | |||
| Pre-exercise | 64 ± 12 | 61 ± 6 | 65 ± 4 |
| Post-exercise | 58 ± 10 c | 57 ± 8 c | 58 ± 5 c |
a Significantly different from both taping styles.
b Significant difference between EAB and NE.
c Significantly different from pre-exercise.
The muscle latency, as measured by surface EMG, did not exhibit any differences between taping styles, but a significant change was noted with respect to pre-exercise and post-exercise testing ( P < .01). All tape conditions showed a reduced latency post-exercise ( Fig. 5 ).
1.3.2
EMG
A repeated-measures Anova indicated that the peroneal longus latency did not differ between tape conditions. The latency decreased significantly after exercise ( P < .001) ( Fig. 6 ).
1.4
Discussion
Our results are in agreement with previous works on this topic . NE taping reduces both ROM and ROI in ankle inversion. Both Ricard et al. and Pederson et al. noted increases in ankle inversion as well as inversion velocity, although the magnitude of the changes was different. Previous work has reported a greater ROM across all conditions, but that may be due to the platform having a greater rotational inversion (37 degrees as compared to our 35 degrees) or to differences between exercise protocols . The results are all in agreement that NE taping does restrain ankle ROM following exercise, as others have reported . Furthermore, we added a third condition, variation of taping style.
As for the ROI, we noted some differences between taping conditions as well as differences before and after exercise. All three conditions showed a significant increase in ROI. The NE version exhibited a significantly lower ROI than did the EAB, noted both before and after exercise. While EAB had a lower ROI than did the control ankle, it was still higher than that observed for the NE taping style. The ROI may be one of the more important effects that ankle taping can exert on the incidence or severity of an ankle sprain. The rate at which the ankle inverts may be one of the key factors resulting in an ankle injury. Other factors that should be considered include the magnitude and direction of the forces and neuromuscular pre-activation . Previous authors have bluntly stated that a lower ROI allows a greater chance for the evertor muscles to respond to the inversion in time to protect the ankle joint . The evertor muscles can develop three times larger moments of force than tape or braces can resist alone at 15° of inversion . The same authors also reported that the addition of tape or a brace can double the force required to further invert the ankle past 15°. They proposed that strong evertor muscles are the best protection against possible ankle inversion injury if the muscles are pre-activated before the foot makes contact with the inverting object .
Since the evertor muscles are also important in maintaining the ankle in a neutral position and thus preventing ankle sprains, we also tested for peroneal longus latency. Although the response time decreased significantly with exercise, there were no differences between tape conditions.
The relevance to ankle sprains is that a muscle requires some time to respond to a perturbation and develop an effective response. Our data showed muscle response times ranging from 56–66 ms. This is consistent with previous authors who have reported latencies of 50–58 ms for the peroneus muscles following unexpected inversion . Adding in the electromechanical delay, and it would take even longer to develop the force needed to evert the ankle. Measured times of 145–153 ms have been reported as an effective total response time . Theoretically, this is the time it would take for the peroneus longus to act in preventing an inversion sprain. Our data shows that peak inversion occurred as quickly as 22 ms in the untaped condition, with a mean of 112 ms, while the NE took an average of 153 ms (prior to exercise) to reach peak inversion. The time to peak inversion for the NE condition was significantly lower than either the EAB or control conditions, while there was no difference between EAB or control. Our results suggest that the NE tape may allow enough time for the peroneal muscle group to act in developing sufficient eversion torque.
The overall results of this study point to the benefits of ankle tape in preventing lateral ankle sprains by limiting the ROI as well as prolonging the time needed to reach maximal inversion. While the taping does not exert an effect on muscle activity, the mechanical delay provided by the tape may be sufficient to allow the evertor muscles to develop the necessary torque to evert the ankle. Ankle taping should be considered a valid means of reducing the risk or severity of lateral ankle sprains.
Disclosure of interest
The authors declare that they have no conflict of interest concerning this article.
2
Version française
2.1
Introduction
De nombreuses études montrent que les traumatismes de la cheville font partie des blessures corporelles les plus fréquentes et entraînent une diminution significative de la participation aux activités physiques . Sur l’ensemble des blessures recensées chez le sportif, 15 % des cas concernent la cheville et les entorses latérales représentent 83,4 % de ces traumatismes de la cheville .
Au vu des données épidémiologiques sur les entorses de cheville, le taping est devenu une pratique commune pour prévenir les traumatismes. En tant que mesure prophylactique, le taping de la cheville a permis de réduire l’incidence ou la sévérité des entorses , à l’inverse un rapport souligne le manque d’effet du bandage sur l’incidence des entorses . Dans la littérature, un débat subsiste sur l’efficacité dans la durée du taping pour le maintien articulaire. Certaines études montrent que celui-ci est considérablement diminué après l’exercice alors que d’autres rapportent que le taping offre une efficacité significative dans la durée pour le maintien articulaire . La raison principale de l’utilisation fréquente du taping semble être sa faculté d’adaptation aux exigences individuelles, qu’elles soient sportives, corporelles ou liées au degré de sévérité de la blessure .
Le taping de la cheville semble réduire le risque de blessure, ou leur gravité, en limitant l’amplitude articulaire et ainsi éviter une mise en surcharge des tissus conjonctifs, par exemple en diminuant l’incidence de blessure par inversion totale ou en réduisant le taux d’inversion .
Il est probable que la limitation de l’amplitude articulaire ne soit pas le seul moyen d’éviter les entorses. La fonction première du muscle long fibulaire est d’assurer l’éversion du pied et peut donc être fortement impliqué dans la prévention des entorses de cheville. Quand le pied part en inversion, le muscle long fibulaire joue un rôle important de mécanisme de défense primaire . En ce qui concerne l’activité musculaire et le soutien externe de la cheville, les données sont contradictoires. Certaines études ont rapporté un effet délétère d’un maintien prophylactique de la cheville sur l’activité musculaire , d’autres publications ne montraient aucun effet significatif sur l’activité musculaire .
Il existe différentes techniques de taping, et elles varient suivant les pays et le type d’activité sportive. Il a été avancé qu’une contention adhésive efficace et adéquate de la cheville est à la fois une science et un art . Certaines méthodes de taping se révèlent obsolètes ou non fondées sur la science, comme dans l’étude de Yamamoto et al. qui rapporte que les nouvelles méthodes de contention adhésive de la cheville offrent un meilleur maintien et une protection plus efficace par rapport aux autres méthodes . On utilise le plus souvent une bande adhésive non élastique (NE) à base d’oxyde de zinc avec un montage à base d’étriers, renfort au talon, montage en huit et verrouillages calcanéens ( heel lock ). La bande NE demande des précautions particulières, tout spécialement quand la technique consiste à appliquer l’adhésif autour d’un membre. Si le taping est trop serré, le risque de garrot augmente ce qui peut entraîner des lésions tissulaires ou même une nécrose des tissus. Dans le meilleur des cas, le confort et la performance peuvent souffrir d’un taping trop serré. Afin d’éviter ces désagréments potentiels, une nouvelle technique de taping utilise une bande adhésive élastique (EAB). Cette technique alternative implique l’utilisation de trois étriers avec un bandage adhésif d’oxyde de zinc comme restriction primaire, suivi d’un montage en 8 avec l’EAB. Le raisonnement étant que l’EAB permet non seulement un maintien adéquat mais autorise également le mouvement fonctionnel sans gêner la circulation sanguine des tissus situés à l’extrémité distale du taping.
Malheureusement, il n’existe pas dans la littérature d’études sur la cinématique, la cinétique et les effets fonctionnels des différents styles de taping. C’est pourquoi l’objectif de cette étude s’attache à répondre à une question fondamentale : existe-t-il une différence entre les types de bandages, EAB et NE, pour le taux d’inversion ou le temps de latence du muscle long fibulaire, avant et après l’exercice ?
2.2
Méthodes
Douze participants volontaires ont été inclus dans l’étude. Tous les participants étaient en bonne condition physique sans pathologie des membres inférieurs. Les sujets ont reçu une information détaillée lors de la collecte de données et ont signé un formulaire de consentement éclairé, approuvé par le comité local d’éthique. Les caractéristiques physiques des patients étaient les suivantes : âge : 24,1 ± 6,8 ans, taille : 174,2 ± 10,1 cm et poids : 76,7 ± 19,9 kg.
Les sujets étaient randomisés dans l’une des trois conditions de taping : un bandage tissé NE, un bandage adhésif élastique (EAB) et un groupe témoin sans bandage ( Fig. 1 et 2 ).

Related posts:
 Is PMR the medical specialty best adapted to today’s issues in public health?
Effects of a low-intensity dynamic-resistance training protocol using an isokinetic dynamometer on muscular strength and aerobic capacity after coronary artery bypass grafting
Rehabilitation and leucine supplementation as possible contributors to an athlete’s muscle strength in the reathletization phase following anterior cruciate ligament surgery
Long-term transanal irrigation’s continuation at home. Preliminary study
Is PMR the medical specialty best adapted to today’s issues in public health?
Effects of a low-intensity dynamic-resistance training protocol using an isokinetic dynamometer on muscular strength and aerobic capacity after coronary artery bypass grafting
Rehabilitation and leucine supplementation as possible contributors to an athlete’s muscle strength in the reathletization phase following anterior cruciate ligament surgery
Long-term transanal irrigation’s continuation at home. Preliminary study
 Sagittal X-ray parameters in walking or ambulating children with cerebral palsy
Sagittal X-ray parameters in walking or ambulating children with cerebral palsy
 Percutaneous treatment of sciatica caused by a herniated disc: An exploratory study on the use of gaseous discography and Discogel ®in 79 patients
Percutaneous treatment of sciatica caused by a herniated disc: An exploratory study on the use of gaseous discography and Discogel ®in 79 patients
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


