Abstract
Urethral diverticulum is a rare pathology in male patients. It is most often encountered in patients with paraplegia due to iterative catheterizations. The diagnosis of a large diverticulum is easy to make when faced with clinical symptoms, such as: repeated urinary tract infections, perineal pain and especially when there is penile swelling. We report the case of a 24-year-old patient with paraplegia and urethral diverticulum. In this case, the issue lies in the therapeutic possibilities.
Résumé
Les diverticules urétraux sont une pathologie rare chez l’homme. Ces derniers sont plus souvent rencontrés chez les patients paraplégiques du fait d’hétérosondages itératifs. Le diagnostic des diverticules importants est assez facilement posé, devant des signes, comme infections urinaires à répétition, douleurs périnéales et surtout devant une tuméfaction à la face inférieure de la verge. Nous présentons le cas de la découverte d’un diverticule urétral chez un jeune homme de 24 ans paraplégique, chez qui le problème posé est surtout thérapeutique.
1
English version
1.1
Introduction
Clean intermittent catheterization is the method of choice for the management of neurogenic bladders. Self-catheterization is the modality of choice and patient education is mandatory. In fact, third-party catheterization can lead to complications, infectious ones but also mechanical ones, such as urethral diverticula which are quite rare but can yield diagnostic and therapeutic problems as shown in our reported case.
1.2
Case report
A 24-year-old patient was sent to our PM&R unit for an evaluation of his paraplegia. He suffers from an undefined congenital neurological disease that associates psychomotor delay and behavioral disorders. In 2007, three months after having been transferred to another care center, the patient fell from a great height. This accident led to complete paraplegia at the level of T12, due to fractures of the T12 and L4 vertebras. Since then, he has been suffering from bladder/bowel disorders with urinary retention alternating with periods of urinary incontinence and leakages that are hard to identify due to the patient’s sensitive and cognitive disorders. He has third-party catheterizations four times a day. Let us note that in 2008, the patient was hospitalized in the urology department for gallstones treatment. Since the beginning of 2010, the act of catheterization became quite difficult. In fact, due to urine leakage between catheterizations, the patient had to wear a penile sheath with urine collector.
Upon admission in our unit, during the examination of the external genital organs, we noted a swelling and bruising in the lower part of the penis, this swelling went down after catheterization. The catheterization draws urine right from the insertion of the catheter down just a few centimeters. The bruising swells up again between catheterizations. The diagnosis of urethral diverticulum seems quite probable.
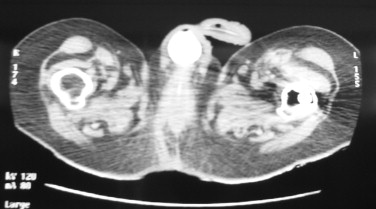
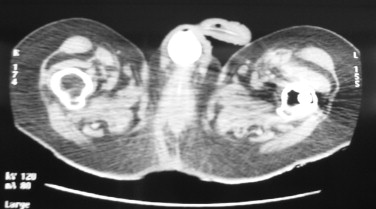
A cystourethrogram and a bladder scan validated this diagnosis highlighting a sub-urethral diverticulum of the penile urethra, measuring 33 mm in diameter (anterior–posterior), 20 mm in width and communicating with the urethra ( Figs. 1 and 2 ).

1.3
Discussion
Urethral diverticula are a rare occurrence in men . Most often, it is due to a formation of a pouch or dilatation at the level of the urethra, most likely from an acquired origin (90%) . They are mostly found at penile level and especially at the penoscrotal angle . The most frequent causes of urethral diverticula are recurrent urinary tract infections (UTIs), long-term catheterization (implanted catheter), trauma of the urethra (recurrent catheterizations or surgical gestures), and iatrogenic wounds of the urethra. They are often seen in patients with paraplegia that tend to develop this pathology due to repeated trauma by long-term third-party catheterizations .
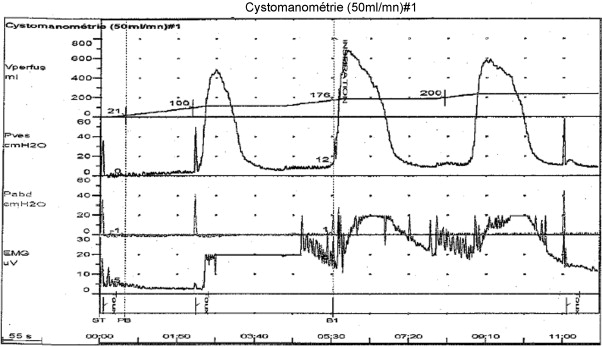
The most common symptoms are: perineal pain, dysuria, urinary incontinence, scrotal edema, a mass on the ventral surface of the external genital organs or perineum, as well as recurrent UTIs . In the case of our patient with a level of injury at T12 and complete paraplegia with spasticity, no sensations were reported during catheterizations (urethral insensitivity) or due to the diverticulum. There was no spontaneous miction and the level of dysuria could not be evaluated. What could have alerted the medical team was the onset of urinary incontinence on a patient that had been stable on a bladder level. In fact, this urinary incontinence was attributed to detrusor overactivity ( Fig. 3 ). In that case, the diagnosis was purely a clinical one, since this large diverticulum could be identified upon palpation. This examination could help define the liquid content in the mass and drain the diverticulum. However, faced with smaller ones, the diagnosis can be quite problematic. In our case, the bladder scan and the cystourethrogram validated the diagnosis avoiding the use of a more invasive exam like cystourethroscopy. If the diagnosis is not possible with the bladder scan, MRI imaging could have been discussed. In fact, MRI is a sensitive and specific examination that can generate cross-sectional images in any plane; it is also quite relevant for the diagnosis of proximal urethral diverticula. Yet, this imaging exam remains costly and not easily accessible . Let us note that this same diagnostic issue is seen in women that, just like men, present non-specific symptoms and in whom there can be concomitant urogenital pathologies .
Regarding the etiological diagnosis for our patient, we were not able to differentiate what was caused by recurrent infections and non-professional third-party catheterizations. The etiology is probably correlated to several factors. If surgery is the treatment of choice for urethral diverticulum to avoid urine leakage, infections, risk of infertility , for our patient, we decided first to implant a supra-pubic catheter. Since this patient, with a detrusor overactivity that was pharmacologically disconnected, requires an instrumental bladder emptying. Due to behavioral disorders, the patient cannot self-manage his catheterization and the problem will be to go back to third-party catheterizations after surgery.
After four months of follow-up, that patient came to the consultation for a purulent urethral discharge and thus a medico-surgical discussion is underway to look at the option of diverticulum surgery while maintaining supra-pubic catheter drainage.
1.4
Conclusion
Urethra diverticula are a rare pathology in men; usually the diagnosis is not problematic, especially faced with large diverticula. However, a rigorous and thorough clinical examination is required. There are however some therapeutic issues depending on the patient’s environment and history, like this dependent patient who requires third-party catheterizations. The latter being in part responsible for the pathology, on mechanical and infectious levels, but they remain essential for bladder management.
2
Version française
2.1
Introduction
Le sondage intermittent propre est maintenant la méthode de référence pour la prise en charge des vessies neurologiques. L’autosondage est la modalité qu’il faut préférer et pour laquelle une éducation est indispensable. En effet, l’hétérosondage n’est pas dénué de complication, infectieuse, mais aussi mécanique, comme le diverticule urétral, qui bien que rare pose des problèmes diagnostiques et thérapeutiques, comme dans le cas rapporté.
2.2
Cas rapporté
Un jeune homme de 24 ans a été adressé à notre service de MPR pour bilan de paraplégie. Ce dernier souffre d’une maladie neurologique congénitale du développement non étiquetée associant retard psychomoteur et trouble du comportement.
En 2007, alors qu’il venait, depuis trois mois, d’être changé d’institution, le patient chute d’une grande hauteur. Cet accident le rend paraplégique de niveau T12 complet, conséquence des fractures des vertèbres T12 et L4.
Il souffre depuis de troubles vésicosphintériens à type de rétention urinaire en alternance avec des périodes d’incontinence urinaire, avec des fuites difficiles à caractériser du fait des troubles sensitifs et cognitifs du patient. Il bénéficie de quatre hétérosondages journaliers par sa tierce personne. À noter qu’en 2008, le patient est hospitalisé en urologie pour traitement de calculs vésicaux.
Depuis début 2010, les hétérosondages deviennent difficiles. En effet, il existe des fuites urinaires entre les sondages rendant nécessaires le port d’un étui pénien avec collecteur d’urines.
À l’entrée dans notre service, à l’examen des organes génitaux externes, on constate une tuméfaction à la face inférieure de la verge, laquelle est rénitente diminuant de volume après les hétérosondages.
Le sondage ramène d’ailleurs des urines dès l’introduction de la sonde de quelques centimètres. La tuméfaction reprend du volume entre les sondages. Le diagnostic de diverticule urétral est alors fort probable.
Une urétrocystographie rétrograde, ainsi qu’un uroscanner confirment ce diagnostic en mettant en évidence un diverticule sous-urétral de l’urètre pénien, mesurant 33 mm de diamètre antéropostérieur, 20 mm d’épaisseur et communicant avec l’urètre ( Fig. 1 et 2 ).
Related posts:
 L’AJMER, représentant des jeunes médecins français de médecine physique et de réadaptation et acteur de leur formation
Boosting disability research in the engineering sciences. The recommendations of the National Observatory for Training, Research and Innovation on Disability (ONFRIH)
The faisability and the effects of cycloergometer interval-training on aerobic capacity and walking performance after stroke. Preliminary study
L’AJMER, représentant des jeunes médecins français de médecine physique et de réadaptation et acteur de leur formation
Boosting disability research in the engineering sciences. The recommendations of the National Observatory for Training, Research and Innovation on Disability (ONFRIH)
The faisability and the effects of cycloergometer interval-training on aerobic capacity and walking performance after stroke. Preliminary study
 Do French medical schools provide appropriate training on gait and gait disorders?
Do French medical schools provide appropriate training on gait and gait disorders?
 Spondylolisthesis on bilateral pedicle stress fracture in the lumbar spine: A case study
Spondylolisthesis on bilateral pedicle stress fracture in the lumbar spine: A case study
 Characterization of an electric stimulation protocol for muscular exercise
Characterization of an electric stimulation protocol for muscular exercise
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


