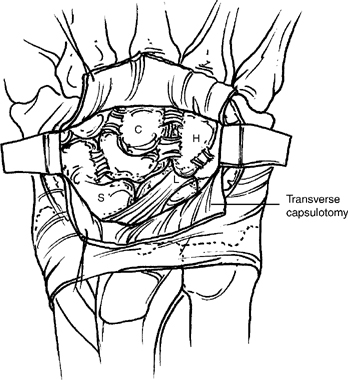
46 Scaphoid Excision with Capitolunate Triquetrohamate Arthrodesis Elderly patients and those with severe wrist stiffness have less predictable pain relief and recovery of motion. Figure 46-1 Incise the distal edge of the extensor retinaculum between the third and fourth compartments to the level of Lister’s tubercle to facilitate exposure. Avoid injury to the radioscaphocapitate ligament, which passes over the palmar surface of the scaphoid waist.
Indications
Pitfall
Technique
Pearl
Pitfall
Related posts:
 Intra-articular Fractures of the Distal Radius Treated with Dorsal Plate
Intra-articular Fractures of the Distal Radius Treated with Dorsal Plate
 Resect Ulnar Styloid Fracture with Repair of Triangular Fibrocartilage Complex
Resect Ulnar Styloid Fracture with Repair of Triangular Fibrocartilage Complex
 Sauve-Kapandji Procedure
Sauve-Kapandji Procedure
 Darrach Procedure (Distal Ulna Resection)
Darrach Procedure (Distal Ulna Resection)
 Scaphocapitate Fusion with Lunate Excision
Scaphocapitate Fusion with Lunate Excision
 Capitate Shortening with Capitohamate Fusion
Capitate Shortening with Capitohamate Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


