Chapter 15 Foot injuries

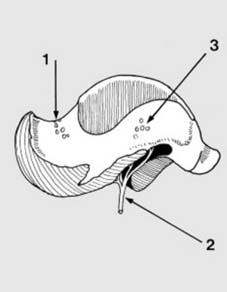

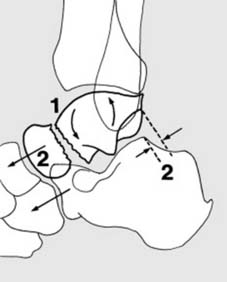


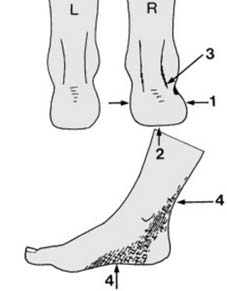
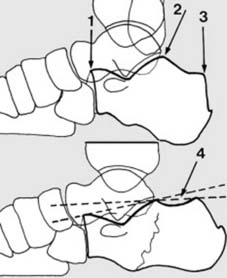
7 Classification (d): Group III injuries: With further dorsiflexion and upward force (1) the tibia is driven between the two talar fragments. The posterior fragment is extruded backwards, while at the same time the convex posterior articular surface of the calcaneus (2) guides it medially. It comes to rest with its medial surface (3) caught on the sustentaculum tali (4).


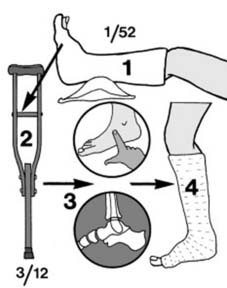

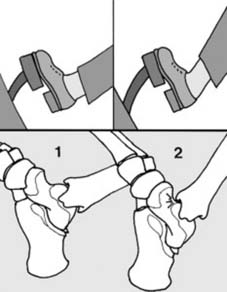
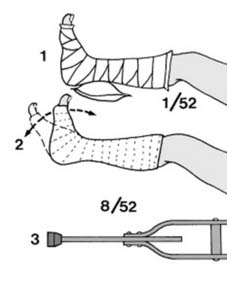
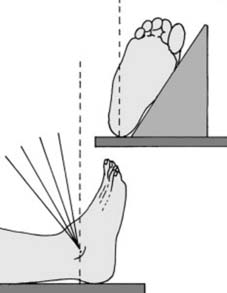
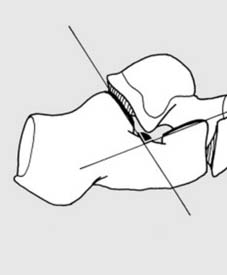
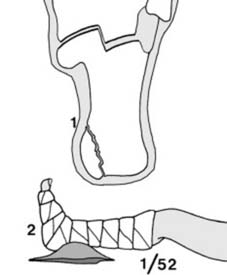
12 Treatment of Type II injuries (a): While some prefer open reduction for all these fractures, closed methods may be attempted: (1) The foot is plantar flexed and everted. (2) A padded plaster is applied in this position and check radiographs taken. If a satisfactory reduction has been obtained, then conservative treatment may be continued.
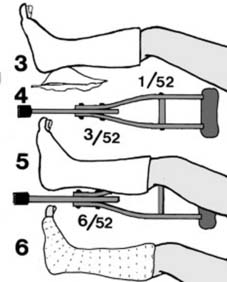



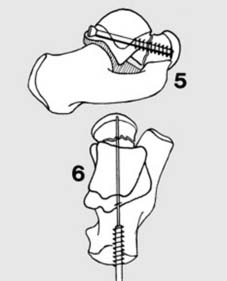
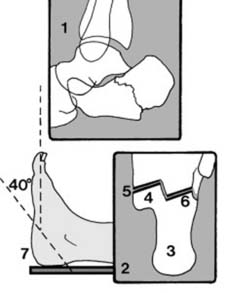
17 Treatment of Group III injuries (c): After reduction, proceed with elevation and gradual mobilisation as described in Frame 13 above. If closed reduction fails (as it often does), open reduction will be necessary. The condition of the skin and any planned internal fixation will dictate the incision(s). These fractures may be fixed (best through a posterolateral incision) with one or two cancellous screws passed from behind through the body of the talus and into the head (5). Cannulated screws may also be used; these can be threaded over Kirschner wires which have been inserted temporarily to hold the reduction (6). The AO group, with an eye to rapid mobilisation, in fact recommend internal fixation along these lines for all talar neck fractures.
Complications of talar neck fractures (a):

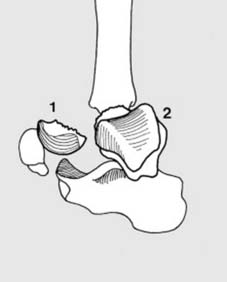
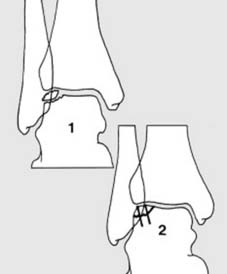
18 Complications ctd: (c) Ankle fracture: Rarely, malleolar fracture may be found complicating talar neck fractures. Closed reduction is here unreliable, and open reduction with internal fixation of the malleolar fracture is desirable. (Illus.: Group III fracture, with fracture of the lateral malleolus.)




23 (c) Avulsion fractures: Minor avulsion fractures of the talus may result from inversion, eversion, plantar flexion and rarely dorsiflexion strains of the ankle – when flakes of bone are pulled off by ligamentous or capsular attachments. These injuries require symptomatic treatment only (e.g. 2–4 weeks in a below-knee walking plaster).



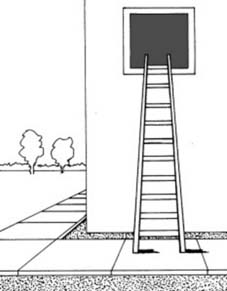
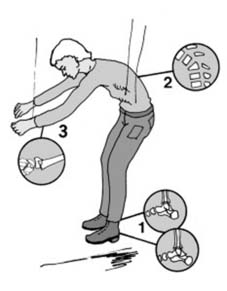
29 Calcaneal fractures: Mechanisms of injury (a): The commonest cause of calcaneal fracture is a fall from a height on to the heels. Important factors include the height fallen, the nature of the ground, and the weight of the patient. The injury is common in slaters, window cleaners and construction workers. Rarely the injury may be produced by impact from below (e.g. a below-deck explosion on a ship).

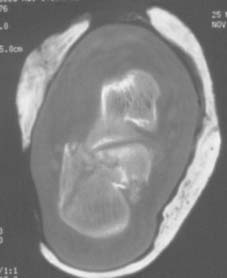
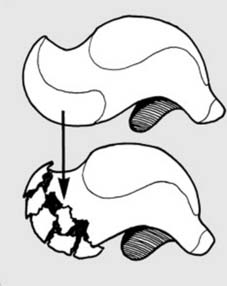
35 Radiographs (d): CT scans can be of value in assessing the nature and degree of comminution of a calcaneal fracture, and any subtalar and calcaneocuboid joint involvement. Coronal, transverse and sagittal projections have all been used. The coronal projection chosen as a standard to allow useful comparison of cases is made through the widest part of the talus. In the scan above the comminution of the calcaneus and involvement of the subtalar joint is obvious.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


