Bone, Joint, and Muscle Problems
Paul D. Sponseller
Most children’s musculoskeletal problems present first to the pediatrician. She/he is entrusted to triage them and sort out those needing observation from those requiring active treatment. This chapter is designed to help in the initial understanding of this broad range of orthopedic conditions. Conditions limited to one body region are presented first, followed by generalized musculoskeletal conditions. Table 432.1 lists the differential diagnosis of certain signs and symptoms and is meant to aid in the formulation of a diagnostic plan.
Because some orthopedic terminology may be a “new language,” a few definitions are in order. The term congenital refers to a condition that is present at birth, regardless of whether it is genetic. Developmental refers to problems that occur or increase with time and growth, irrespective of their causes. The regions of a long bone have specific names. Physis refers to the growth plate (Fig. 432.1); therefore, the epiphysis is that portion of a bone “on top of” the physis (i.e., nearer to the joint), the metaphysis is the widened portion of the shaft adjacent to and arising from the growth plate, and the diaphysis is the narrow portion of a tubular bone midway between two physes. Another set of terms refers to joints and their geometric relationships. The Greek root words genu, coxa, and pes refer to the knee, hip, and foot, respectively. They are used in such terms as genu recurvatum (hyperextensible knee), coxa plana (flat femoral head [i.e., Perthes disease]), and pes planus (flat feet). When two bones or two fracture fragments form an angle, they are in varus when the apex of the angle points away from the midline of the body, and they are in valgus when it points toward the midline (Fig. 432.2). Alternatively, angulation may be stated by the direction of the apex (i.e., genu valgus is a medial angulation of the lower extremity at the knee). Dislocation refers to complete loss of contact of two joint surfaces, and it is specified by the direction of displacement of the most distal part. For example, most shoulder dislocations are anterior because the humeral head comes out in front of the scapula. Subluxation is an incomplete dislocation. Abduction refers to movement away from the midline of the body; adduction denotes movement toward the midline.
One of the themes of this chapter is the changing nature of the skeleton with growth. Many clinical findings improve with time, due to the normal remodeling processes under the influence of growth and muscle forces: genu valgum, metatarsus adductus, tibial torsion, and fracture angulation. Others may get worse, such as Blount disease, neuromuscular hip dysplasia, and severe idiopathic scoliosis. Experience and judgment are needed to make these distinctions.
REGIONAL ABNORMALITIES
Hip and Femur
Developmental Dysplasia of the Hip
The normal hip develops from a single area of cartilage that then forms a joint cavity. Its characteristic spherical shape results from reciprocal contact and movement between the femoral head and acetabulum during in utero development. Loss of this contact may occur as a result of abnormal in utero positioning; such neuromuscular abnormalities as cerebral palsy, arthrogryposis, and Larsen syndrome; or intrinsic underdevelopment of the otherwise normal hip. The earlier an abnormal positioning occurs, the more marked are the femoral and acetabular abnormalities that result; the later it is corrected, the less is the remodeling potential.
The cause of congenital dislocation of the hip in an otherwise normal child is multifactorial. Mechanical factors play a role; thus, the frequency is increased greatly in fetuses with breech presentation, a factor in 30% of all cases of developmental dysplasia of the hip (DDH) in firstborn children and in infants with oligohydramnios. The left hip is involved more commonly than is the right. These factors cause positioning in adduction and hyperflexion, leading the femur to be directed out over the edge of the acetabulum. Hormonal factors may play a role, because generalized ligamentous laxity occurs around the time of birth, caused by an increase in circulating estrogens and relaxin. Probably for this reason, the incidence of DDH is sixfold greater in girls than in boys. More than 20% of patients have a positive family history.
TABLE 432.1. DIFFERENTIAL DIAGNOSIS OF COMMON PEDIATRIC SYMPTOMS | |
|---|---|
|
In order of their increasing severity, the three degrees of hip dysplasia are subluxable, dislocatable, and dislocated. In the subluxatable hip, the femoral head rests in the acetabulum and can be dislocated partially during the examination. The dislocatable hip can be dislocated fully with manipulation but is located normally when a baby is at rest. In the dislocated hip, the femoral head rests in the dislocated position. The combined incidence of these three conditions is 1 in 60 births; the incidence of true dislocation is only 1 to 2 per 1,000 births. The term dysplasia describes the spectrum of severity of this disorder, which ranges from slight malformation to full dislocation of the hip. The term developmental acknowledges that some cases cannot be detected at birth and may occur later. The pathologic anatomy includes capsular laxity. Also, the acetabulum becomes shallow as a result of lack of contact with the femoral head. A false acetabulum may form where the femoral head contacts the pelvis above the normal location. The outer rim of the acetabulum becomes rounded during the period when the femoral head is able to slide in and out of the acetabulum. The movement over this ridge is felt as the “clunk” of the Ortolani and Barlow tests. The femur remains rotated anteriorly (anteverted) as the head rests against the lateral iliac wall.
Physical examination remains the key to the diagnosis of DDH. The signs in the newborn period usually include instability without significant fixed deformity; in later months, untreated dislocation becomes more fixed, and less instability and more limitation of certain motions occur. Specifically, Barlow and Ortolani signs should be sought in newborns. These signs are defined as positive when the hip can be dislocated and relocated, respectively. Infants should be relaxed when the tests are performed, and only one hip should be examined at a time. The pelvis should be stabilized with one hand while the femur is controlled with the other hand, with fingers placed on the greater and lesser trochanters (Fig. 432.3). With adduction and pressure directed posteriorly, the femur can be felt to slide “out” in a posterosuperior direction in the abnormal hip (Barlow sign; see Fig. 432.3A) and then back in with abduction, causing a dull clunk to be heard (Ortolani sign; see Fig. 432.3B). Thus, the Barlow and Ortolani signs, which are the
sensations of dislocation and relocation, are alternate phases of the same process of hip instability.
sensations of dislocation and relocation, are alternate phases of the same process of hip instability.
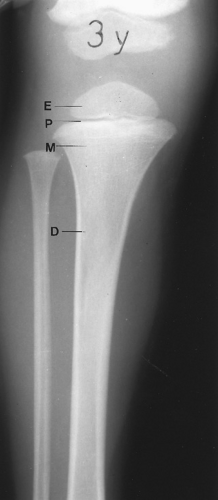 FIGURE 432.1. Regions of a long bone. D, diaphysis; E, epiphysis; M, metaphysis; P, physis. |
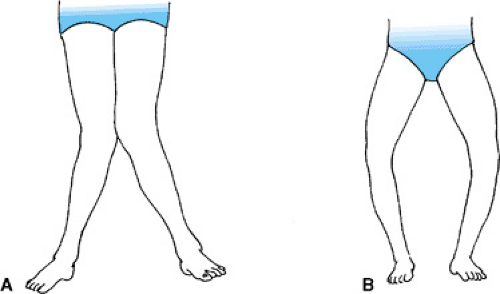 FIGURE 432.2. Examples of varus and valgus. A: Genu valgus, because apex of angulation is toward midline. B: Genu varus. |
A common error made in DDH diagnosis is examining both hips at once, which impairs sensitivity. Another error is mistaking insignificant soft tissue “clicks” for the more important and palpable “clunk.” These innocent clicks may result from movement of fascia over the greater trochanter or may originate from the meniscus of the knee or the patella. Routine screening of neonates in the last three decades has resulted in a dramatic increase in the early diagnosis of DDH and, thus, more successful treatment of the disorder.
Approximately 60% of all unstable hips seen in newborns normalize spontaneously within the first 2 to 4 weeks after birth as the baby is free of the constraints of the womb and perinatal laxity resolves. Not all hips can be reduced at birth, however, presumably because of fixed joint contracture. Some cases of dysplasia are believed to develop after birth. For this reason, most large series have shown that not all abnormal hips can be detected by screening, even when it is performed by skilled examiners. Neonatal ultrasonography is a useful tool in examining a newborn’s hip, but it does not provide the precise image that we are accustomed to see in a radiograph or magnetic resonance imaging (MRI). It is much less clear than a prenatal ultrasound, because of the lack of a uniform fluid medium. It may result in overdiagnosis of dysplasia if performed on all newborns. Recommended indications for ultrasonography vary from region to region, but they usually involve some combination of abnormal physical examination or presence of risk factors.
 FIGURE 432.3. Barlow and Ortolani tests, performed with fingers on the lesser and greater trochanters, examining only one hip at a time. A: Barlow test: adduction and posterior pressure may produce a “clunk” of subluxation or dislocation. B: Ortolani test: abducting and “lifting” hip back into place. C: In children older than 3 to 6 months, Barlow and Ortolani tests often will be negative despite dislocation because of diminished laxity; the most important finding in this age group may be limitation of abduction. |
The signs of a dysplastic hip change with time. If the hip remains dislocated, usually it cannot be relocated in the awake state by the time an affected baby is 6 months old. Findings of asymmetry, such as a limitation of abduction (see Fig. 432.3C) and apparent shortening of the thigh, are more sensitive at this time. This last sign, known as Allis sign or the Galeazzi sign, is best noted by comparing the lengths of the two flexed thighs when they are held together. Asymmetry of skin folds by itself is an unreliable finding. When children begin to walk, a positive Trendelenburg sign is noted: When weight is borne on the unstable side, the pelvis drops to the other side.
Radiographs are not the preferred imaging method before age 6 months because of a lack of easily detectable bony changes during this time, except in infants with teratologic conditions. Many centers use ultrasonography, but the accurate interpretation of these studies requires extensive experience and should be done by a pediatric radiologist or orthopedist. Ultrasonography is indicated if the neonatal examination is abnormal or questionable, and it may be used later to guide treatment. After age 6 months, the increasing ossification of the femur renders ultrasonography less reliable, and plain films are preferred. Anteroposterior (AP) radiography of the pelvis may show cephalad and lateral migration of the femur with a break in Shenton’s line (Fig. 432.4), delayed appearance of the femoral ossific nucleus, a shallow and more vertical acetabulum, and later formation of a false acetabulum.
Treatment is more complex as age increases. The aim of all therapy is to restore contact between the femoral head and the acetabulum. Because a high percentage of patients experience spontaneous improvement of lax hip capsules in the early perinatal period, most orthopedists recommend observing a hip that is subject to subluxation and reexamining it at age 3 to 4 weeks. Dislocated hips should be treated at the time of diagnosis. Usually, the initial treatment is a brace that holds the hip in flexion and abduction, such as the Pavlik harness, which allows some motion while it holds the hip reduced. The alignment should be checked by ultrasound in 1 to 2 weeks. The brace is worn until the clinical and radiologic examinations are normal, an interval equal to approximately one to two times an affected child’s age at diagnosis. If treatment is begun after affected children have reached age 6 months, usually they are too large and strong to tolerate the brace. At that point, reduction is performed under general anesthesia. Sometimes this procedure has been preceded by a period of traction to stretch out the soft tissues. Closed reduction is attempted first and checked with an arthrogram. If it is successful, the reduction is held in a spica cast for a number of months. If closed reduction is unsuccessful, open reduction should be performed.
Open reduction involves releasing the tight psoas tendon and inferior capsule, thus allowing the femoral head to be brought down to its appropriate location.
Open reduction involves releasing the tight psoas tendon and inferior capsule, thus allowing the femoral head to be brought down to its appropriate location.
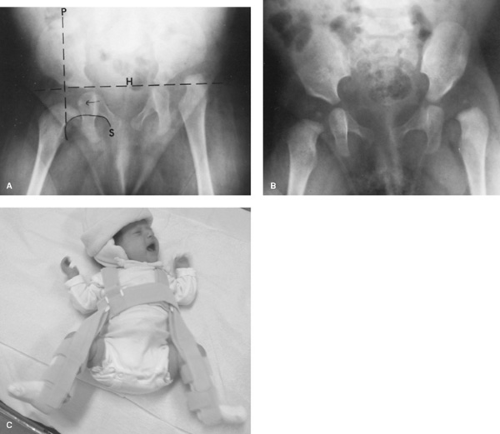 FIGURE 432.4. A: Illustrations of a congenitally dislocated hip. The femoral head ossific nucleus should be within the lower inner quadrant formed by Perkin’s vertical line (P) at the outer edge of the acetabulum and Hilgenreiner’s horizontal line (H). The nucleus appears at age 5 months, on the average. Shenton’s line (S) is the arc of the femoral neck, which should continue smoothly into the superior pubic ramus. This is a teratologic hip dislocation; note extreme height and rounded false acetabulum. B: A subtler example of congenital dislocation of the left hip. C: Infant with congenital hip dislocation treated in a Pavlik Harness. |
If extensive distortion of the bones (i.e., a shallow acetabulum or a rotated femur) has occurred, a femoral or pelvic osteotomy and open reduction might be indicated. This condition is more common in patients who are older than 2 years.
Possible complications include persistent dysplasia from failure of normal development, recurrent dislocation, and avascular necrosis of the femoral head. The latter condition, which is the most serious complication of DDH, is caused by obstruction of the epiphyseal vessels by excess pressure or capsular stretch.
The earlier that treatment is carried out, the better is the resultant hip development and the safer is each of the steps in treatment. Thus, careful, methodical early screening can decrease the need for complex orthopedic procedures later.
Transient (Toxic) Synovitis of the Hip
Transient (toxic) synovitis of the hip is a diagnosis of exclusion; this self-limited condition is the most common cause of an irritable hip in children. The usual clinical presentation is a painful limp or hip pain of acute or insidious onset, usually occurring unilaterally. The most common age range for the condition is 2 to 6 years, but it has been described in patients ranging from ages 1 to 15. Spasm occurs on testing of hip range of motion, particularly with internal rotation. The temperature, white blood cell (WBC) count, and erythrocyte sedimentation rate may be normal or slightly elevated. The cause of the condition is unknown; an immune mechanism or viral infection is postulated. The differential diagnosis should include septic arthritis, osteomyelitis, and Legg-Calvé-Perthes disease, which usually is associated with changes in the femoral head on radiography. Juvenile monoarthritic rheumatoid arthritis and slipped capital femoral epiphysis (SCFE) also should be considered. Admission to the hospital, observation, and possible early aspiration should be undertaken if septic arthritis cannot be ruled out. Treatment consists of bed rest, with analgesic agents provided as needed for 2 to 7 days. Sometimes, if the diagnosis is clear, therapy can be accomplished on an outpatient basis with frequent follow-up. Persistence of the symptoms beyond 1 week should prompt reevaluation, although bed rest for as long as 1 month occasionally has been required.
Legg-Calvé-Perthes Disease (Coxa Plana)
The cause of Legg-Calvé-Perthes disease still is unknown. More recent evidence indicates that some cases may be caused by a subclinical hypercoagulable state, such as a deficiency of antithrombotic factors S or C or a decrease in fibrinolysis. The condition is characterized by ischemic necrosis of the proximal femoral epiphysis, with later resorption and eventual healing. The amount of the femur that is rendered ischemic varies and affects the outcome. Ischemia is followed by reossification, with or without collapse of the femoral head. Legg-Calvé-Perthes disease usually, but not exclusively, affects children between ages 4 and 8. Boys are affected four times as often as are girls. As a group, affected patients have slightly shorter stature and delayed bone age as compared to their peers. Fifteen percent of all cases are bilateral.
Usually, the clinical presentation of this disorder is a limp (i.e., an abductor lurch) with minimal pain of either short or long duration. The pain is not as acute or severe as that of transient synovitis or septic arthritis. In some patients the pain may be referred to the thigh or the knee. Motions that are especially limited include internal rotation and abduction. Internal rotation is tested with the patient supine and the hip flexed, and the angle to which the leg may be rotated laterally is measured. These movements may be resisted by mild spasm or guarding. In the earliest stage, radiographic results may be normal or reveal that the affected femoral epiphysis is slightly smaller when compared with the contralateral side, as a result of its failure to grow after becoming avascular. Later, a narrow crescentic lucency, seen best on the lateral view, may be observed; it is the result of a tiny fracture of the subchondral bone. This view reveals the extent of bone involved (Fig. 432.5A). In some cases, revascularization may occur without collapse; in others, revascularization of the femoral head is accompanied by progressive resorption and deformation, often with lateral and superior migration (Fig. 432.5B). Reossification follows, and the femoral head continues to grow (Fig. 432.5C). Whether this further growth occurs spherically depends on the patient’s age, the amount of collapse, and the method of treatment.
The differential diagnosis should include transient synovitis, septic arthritis, hematogenous osteomyelitis, various types of hemoglobinopathy, hypothyroidism, and the epiphyseal dysplasias. Often, the latter two conditions are temporally symmetric bilaterally, whereas Legg-Calvé-Perthes disease is not.
Treatment follows two principles: containment of the femoral head within the acetabulum and maintenance of range of motion. During the vulnerable phase, the avascular portion of the femoral head is less likely to become deformed severely and is more likely to reconstitute spherically if it is contained within the “mold” of the acetabulum by abduction. Children younger than 6 years or those who have involvement of less than one-half the femoral head may be observed without active treatment if a full range of motion is preserved, because this range signals containment, and patients in this age group have a good prognosis. Aggressive treatment is indicated for patients who have involvement of more than one-half the femoral head and are older than 6 years.
Containment may be achieved by surgery. Either a femoral osteotomy to redirect the involved portion within the acetabulum or an innominate osteotomy or shelf procedure may be performed (Fig. 432.6). The two procedures produce approximately equal results. Surgery does not speed the healing of the femoral head, but causes it to reossify in a more spherical fashion. Generally, children with Legg-Calve-Perthes disease have intermittent mild aching in the hip for 1.5 to 2 years, until reossification is complete, but then they are virtually asymptomatic throughout childhood. Arthritic symptoms may develop later in adulthood, depending on the degree of this deformation.
Slipped Capital Femoral Epiphysis
SCFE is a growth-plate disorder that occurs near the age of skeletal maturity; it involves a displacement of the epiphysis posteriorly, medially, and inferiorly. In other words, the femur is rotated externally from under the epiphysis. Usually, SCFE occurs without severe sudden force or trauma. The cause appears to involve both mechanical and biologic factors. Mechanically, in most affected children, increased stress occurs as a result of obesity and abnormal retroversion (posterior rotation) of the femoral head and neck. The periosteum at this age is thin and less able to resist the shearing forces. Possible biologic causes include hormonal factors and delayed growth-plate maturation. Increased growth hormone levels have been associated with decreased physeal shear strength, and hypothyroidism has been found in some cases. Usually, in girls, SCFE occurs during the growth spurt and before menarche. The condition is rare, with a frequency of 1 in 100,000 to 8 in 100,000. It is more common in boys and in African Americans. Approximately one-fourth to one-third of all affected children experience bilateral involvement, but usually not simultaneously.
The clinical presentation varies with the acuity of the process. Most affected children exhibit a limp and endure varying
degrees of aching or pain. The discomfort may be in the groin, but often it is referred to the thigh or knee. This variation may cause confusion: Many patients are dismissed for an apparent knee complaint with no obvious cause, only to have the true hip pathology discovered later with worsening of the slip. This paradoxic distribution of pain is attributed to referral within the femoral nerve distribution, which involves both the hip and knee joints. Abduction, internal rotation, and flexion are the motions that are most limited. A characteristic finding is external rotation of the hip with flexion, which is caused by the preexisting retroversion and the slip itself (Fig. 432.7). Some patients have acute, severe pain and an inability to walk or move the hip. This is termed an “unstable” slip and indicates an increased risk of avascular necrosis.
degrees of aching or pain. The discomfort may be in the groin, but often it is referred to the thigh or knee. This variation may cause confusion: Many patients are dismissed for an apparent knee complaint with no obvious cause, only to have the true hip pathology discovered later with worsening of the slip. This paradoxic distribution of pain is attributed to referral within the femoral nerve distribution, which involves both the hip and knee joints. Abduction, internal rotation, and flexion are the motions that are most limited. A characteristic finding is external rotation of the hip with flexion, which is caused by the preexisting retroversion and the slip itself (Fig. 432.7). Some patients have acute, severe pain and an inability to walk or move the hip. This is termed an “unstable” slip and indicates an increased risk of avascular necrosis.
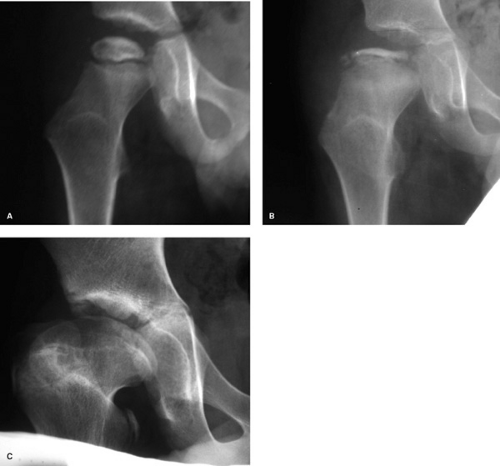 FIGURE 432.5. A: Early Legg-Calvé-Perthes disease, showing early flattening of the femoral head. B: Later, further resorption and apparent collapse of the femoral head are evident. C: Finally, restoration of a slightly ovoid but fully ossified femoral head is seen here at age 13, although the femoral neck is slightly short. |
The earliest radiographic findings are widening and irregularity of the growth plate and osteopenia of the femur. Later, displacement of the epiphysis occurs and is seen best on the frog-leg lateral view of the pelvis. On the AP view, a line drawn through the upper margin of the narrowest portion of the neck should intersect at least 20% of the epiphysis (Fig. 432.8). This point is important because, with remodeling during chronic slipping, a step-off at the junction of the epiphysis and metaphysis may be absent. The severity of the slip is graded as mild (less than 33%), moderate (33% to 50%), or severe (greater than 50%). Later changes may include avascular necrosis of the epiphysis or chondrolysis (i.e., joint-space narrowing).
Treatment centers on preventing further slippage, usually by placing affected patients immediately at bed rest and obtaining a prompt orthopedic consultation. Surgery is intended to stabilize the upper femur and to cause the growth plate to close, thereby eliminating the weakened zone. Realignment of the slip is not safe in chronic cases, because the forces necessary to accomplish realignment may produce avascular necrosis by disrupting the blood supply to the epiphysis. The standard treatment is screw fixation in situ. The screw should not penetrate the joint. Osteotomy of the proximal or distal neck to correct the deformity has been performed occasionally, but it carries a high risk of avascular necrosis.
The contralateral side should be monitored by affected patients’ parents for symptoms of SCFE and should be pinned
early if such symptoms occur. Long-term follow-up reveals no early degenerative change unless chondrolysis or avascular necrosis occurs; each has an incidence of 1% to 5% and produces disability during adolescence. However, even in the absence of these complications, degenerative joint disease may occur in middle age.
early if such symptoms occur. Long-term follow-up reveals no early degenerative change unless chondrolysis or avascular necrosis occurs; each has an incidence of 1% to 5% and produces disability during adolescence. However, even in the absence of these complications, degenerative joint disease may occur in middle age.
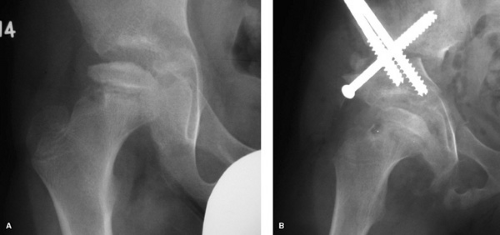 FIGURE 432.6. Operative containment for Perthes disease in an older child. A: Preoperative radiograph shows resorption of bone from femoral epiphysis and partial extrusion from acetabulum. B: postoperative radiograph shows acetabulum rotated to cover femoral head. This is an example of an iliac osteotomy. |
Increased Femoral Anteversion
Increased femoral anteversion causes toeing-in and is one of a spectrum of torsional deformities that affect the alignment of the knee and foot. The differential diagnosis of toeing-in includes this disorder and internal tibial torsion and foot deformities, such as metatarsus adductus (see Table 432.1). Increased anteversion of the femur is defined as an increase in the angle between the plane of the femoral neck and the plane of the knee (posterior femoral condyles; Fig. 432.9). Normally, this angle is approximately 30 degrees at birth and declines to 15 degrees by age 10. Femoral anteversion persists in some neuromuscular conditions, presumably as a result of lack of remodeling forces. The type discussed here is isolated idiopathic femoral anteversion.
 FIGURE 432.7. In slipped capital femoral epiphysis, the hip rotates externally as it is flexed by the examiner. |
On physical examination, affected patients appear to toe in unless compensatory external tibial torsion is present. The patellae also face medially (“squint”). Internal rotation of the hip is much greater than is external rotation in both flexion (supine) and extension (prone). Usually, anteversion is not clinically significant unless external rotation at the hip is less than 15 degrees.
Radiographically, the femoral head and neck appear to be relatively straight on an AP film, with the patella forward. This is a one-plane projection of a two-plane deformity. Computed tomography (CT) is the best device for measuring femoral anteversion directly.
The natural history of femoral anteversion is benign. In a few patients, it may contribute to patellar malalignment. Anteversion later in life has been found to be unrelated to arthritis of the hip or knee. Anteversion does not impair function. Treatment of increased anteversion consists of observation, at least until affected patients are age 8, and restriction from prolonged W-sitting (with the knees touching and the legs folded under), which may impair remodeling. Instead, affected children should sit in the tailor position (with the feet tucked under and the knees out to the side). Braces and bars are not effective in derotating the femur, and no orthotic method of treatment affects anteversion. In fact, most cases need no treatment.
Femoral osteotomy, proximally or distally, is the only way to realign the femur. It should be performed rarely, however, and only in children who are older than 8 and have functional disability as a result of patellar malalignment or, rarely, a persistent concern regarding their appearance.
Knee
Extensor Mechanism Disorders (Patellofemoral Problems)
The patellofemoral joint is subject to repeated high loads of laterally and posteriorly directed forces. Numerous conditions
involving this joint have been described in children and adolescents, and they are treated by attempting to improve the basic forces.
involving this joint have been described in children and adolescents, and they are treated by attempting to improve the basic forces.
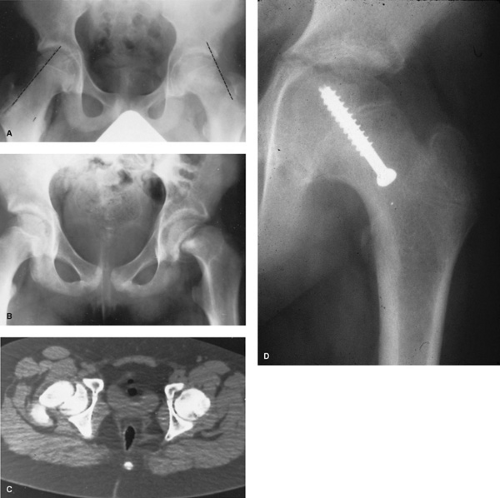 FIGURE 432.8. Radiographic findings in slipped capital femoral epiphysis. A: A line drawn along the superior-lateral femoral neck intersects less than the normal 20% of the epiphysis on the left (affected) side. B: A more severe slip, showing that the femoral neck subluxates laterally and superiorly with respect to the epiphysis. C: Computed tomographic scan most clearly shows the direction of the slip. D: This figure shows in situ fixation of slipped capital femoral epiphysis with a single screw, the preferred method for slips of mild to moderate degree and even many cases of severe degree. |
Chondromalacia refers specifically to the appearance of softening and degeneration of the patellar cartilage. Patellar subluxation refers to partial lateral displacement of the patella. The terms patellofemoral stress syndrome, patellar malalignment, and excessive lateral pressure syndrome refer to the abnormal mechanics causing stress concentration and pain.
The patellofemoral force may be as great as 2.5 times body weight and is greatest with the knee in flexion. The average tibiofemoral angle is approximately 6 degrees outward, which the patella must follow. The quadriceps-patella mechanism itself is angled away from the midline of the body, as measured by the Q (quadriceps) angle from the anterosuperior spine to the patella to the tibial tubercle (Fig. 432.10A). These high forces and asymmetric loads cause minor variations to become significant, especially when repeated over the high numbers of cycles that occur as a part of daily living. Possible factors contributing to patellar pathology (Fig. 432.10B) include increased outward angulation of the knee, abnormal rotation in the form of increased anteversion of the femur or external torsion of the tibia, a high patella (“alta”), abnormal shape or development of the quadriceps, or flattening of the femoral groove. Laxity of the medial side of the patellar restraints contributes to subluxation or dislocation. Normally, women have slightly greater genu valgum than do men. Usually, the aforementioned factors cause greater stress on the lateral side of the patella and, sometimes, decreased medial patellofemoral contact. Cartilage degeneration occurs as a result of the decreased contact.
Clinically, problems with the patella cause aching that is greatest in the anteromedial knee region, on the medial side or center of the patella. Usually, this pain is worse with stair climbing or prolonged sitting, as flexion increases patellofemoral
force. Crepitus may be felt, but it may be painless in some patients and is not pathologic in itself. “Catching” or “locking” may be noted and might represent pain-induced inhibition or mechanical phenomena. A feeling of “giving way” may be described by the patient, especially with subluxation of the patella.
force. Crepitus may be felt, but it may be painless in some patients and is not pathologic in itself. “Catching” or “locking” may be noted and might represent pain-induced inhibition or mechanical phenomena. A feeling of “giving way” may be described by the patient, especially with subluxation of the patella.
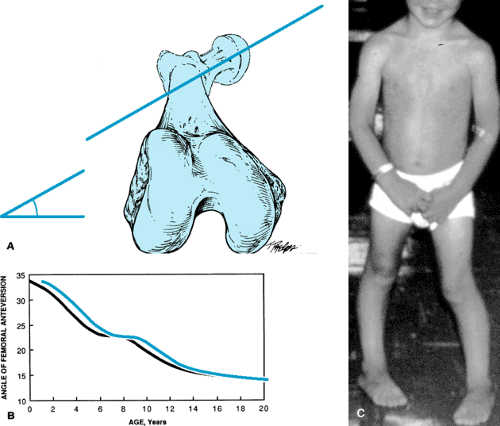 FIGURE 432.9. A: Femoral anteversion is defined as the rotation of the femoral neck forward (in comparison with the distal condyles), as seen in this view down the axis of the femur. B: The curve shows the normal decrease in femoral anteversion with age. C: Child with femoral anteversion, showing inward position of knees as well as feet. |
On physical examination, the most reliable way to test patellar tenderness is by direct compression of each facet against the femur. Palpation under the patella is not diagnostic. Contraction of the quadriceps and patella against resistance is nonspecific because it may be painful even in normal persons. Effusion is present only if patellar degenerative changes or extreme overuse has occurred. Reproducing patellar subluxation with laterally directed pressure may cause apprehension. The Q angle, femoral anteversion, and tibial torsion should be checked. Usually, radiographic results are nonspecific, but lateral displacement or tilt of the patella may be seen occasionally on the sunrise view.
The natural history of patellofemoral stress disorders is that they are common in patients between the ages of 10 and 20, but often they become less symptomatic later. Usually, they do not progress to osteoarthritis.
The differential diagnosis includes a synovial fold or “plica” that may snap over the medial femoral condyle, a medial meniscus tear, tendinitis of the quadriceps or patellar tendon, or osteochondritis dissecans of the patella or distal femur.
Treatment consists of altering the abnormal stresses that are occurring. Patients should refrain from activities performed with the knees flexed, especially those that cause pain (i.e., stair climbing, prolonged sitting, and bicycling). Temporary rest from sports and the use of nonsteroidal antiinflammatory agents may be necessary. Exercises to strengthen the medial (stabilizing) part of the quadriceps include resisted extension from 0 degrees to 30 degrees, most practically by lifting weights within this range or extending the knee on a pillow, flattening it. Hamstrings and rectus femoris muscles, if they are tight,
should be stretched to decrease preload on the extensors. Arch supports may help if severe flexible flatfoot is contributing to tibial torsion. Surgical measures include release of a tight lateral patellar retinaculum, medial soft tissue tightening, tibial tubercle transfer, or correction of genu valgum, knee anteversion, or patella alta if it is severe; all produce satisfactory pain relief in 75% to 90% of patients.
should be stretched to decrease preload on the extensors. Arch supports may help if severe flexible flatfoot is contributing to tibial torsion. Surgical measures include release of a tight lateral patellar retinaculum, medial soft tissue tightening, tibial tubercle transfer, or correction of genu valgum, knee anteversion, or patella alta if it is severe; all produce satisfactory pain relief in 75% to 90% of patients.
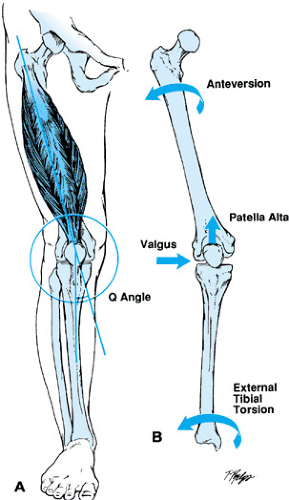 FIGURE 432.10. A: The Q angle, measured from anterior superior iliac spine to center of patella to tibial tubercle. B: Factors that may contribute to excess patellofemoral stress. |
Patellar dislocations may be acute, recurrent or, rarely, habitual. Almost always, they occur in the lateral direction. Acute dislocations are associated with significant swelling and medial knee pain and with a history of significant outward or rotating force. They should be treated with a lateral knee immobilizer until symptom-free, except in skeletally mature patients with bony avulsion. Recurrent subluxation is common, causes less pain and swelling, and often occurs with minimal force. Usually, an associated extensor mechanism abnormality is present. A realignment operation (as described) is the only effective way to stop frequent and bothersome episodes.
Variously, Osgood-Schlatter disease, patellar tendinitis (jumper’s knee), and quadriceps tendinitis are manifestations of excessive, repetitive stresses on the extensor mechanism. They are listed here in order of decreasing frequency in children.
Osgood-Schlatter Disorder
Osgood-Schlatter disorder is a traction-induced inflammation of the tibial tubercle. It is a reaction of the bone and cartilage of this region to high stress. The tibial tubercle is a downward extension of the proximal tibial epiphysis. It develops an ossification center in patients between ages 9 and 13 years, but it does not ossify completely until they are 15 to 17 years old. Within this age range, repetitive stresses gradually can deform the outer surface of the tubercle, causing it to enlarge and become locally inflamed (Fig. 432.11). Tenderness and swelling are localized to this region. Symptoms are worse with running, jumping, or kneeling. Treatment involves decreasing activity to a tolerable level and occasionally using a knee immobilizer, crutches, and ice after activity in severe cases. The patient may be vulnerable to recurrence of symptoms for up to 2 years until the tubercle matures. If affected children and their families are informed of this likelihood, individual regulation of activities can be effective. Usually, activities of daily living and even some sports are tolerated, using daily stretching of tight quadriceps and hamstrings and occasional antiinflammatory agents. Complete avulsion of the tubercle is extremely rare and seems to be related more to sudden stress than to apophysitis.
Patellar Tendinitis
Inflammation at the origin of the patellar tendon (which is at the inferior pole of the patella) is known as patellar tendinitis and is related to the same type of overuse as that seen in Osgood-Schlatter apophysitis. Most often, it is seen in basketball players and also is called jumper’s knee. The duration of pain serves as a guide to the severity of involvement. Pain that is present during both rest and activity is more worrisome than is pain that occurs only after activity. Treatment is the same as that for Osgood-Schlatter disorder. Warm packs before and cold packs after activity also may be beneficial. Rarely, pain may occur at the proximal pole of the patella; in this case, the condition is termed quadriceps tendinitis. Treatment is the same as that described for Osgood-Schlatter apophysitis.
Tibiofemoral Disorders
Popliteal Cysts
Popliteal cysts in children are localized behind the knee on the medial side (Fig. 432.12). They are firm and nontender, vary in size with activity, and transilluminate in a darkened room. They occur most commonly in boys younger than age 9. The origin of these cysts is a slitlike communication between the knee joint and the gastrocnemio-semimembranous bursa. Unlike those in adults, in children, usually these cysts are not associated with any intraarticular pathology, and they tend to resolve spontaneously with time. Actually, the recurrence rate is higher after surgical excision.
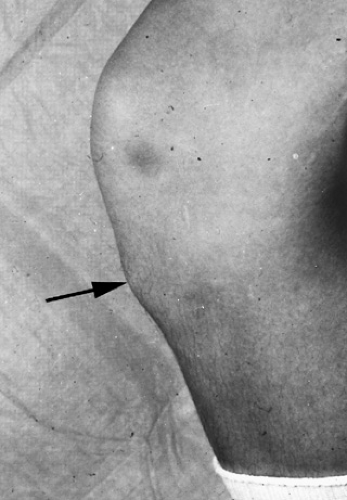 FIGURE 432.11. Osgood-Schlatter disease often produces an enlargement of the tibial tubercle (arrow). |
Discoid Meniscus
An acquired flattening of the lateral meniscus is known as discoid meniscus. In some cases, this flattening occurs as a result of the absence of normal peripheral attachments. Often, such symptoms as pain, clicking, and locking develop in the absence of trauma in children from the age of 2 to adulthood. The meniscus should be trimmed or excised if symptoms become severe. If the attachments are intact, no removal is necessary unless a tear is seen.
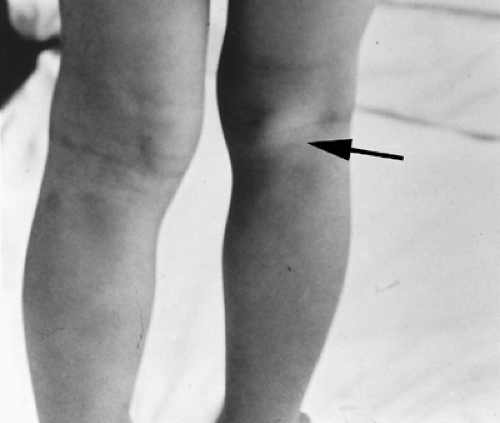 FIGURE 432.12. Popliteal cyst (arrow) in typical (medial) location behind right knee of this child. |
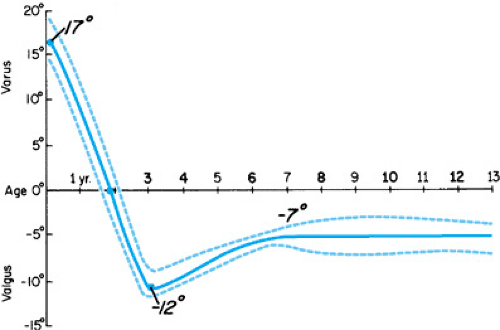 FIGURE 432.13. Normal change in the tibiofemoral angle during growth. (Reproduced with permission from Salenius P. Development of the tibiofemoral angle in children. J Bone Joint Surg 1975;57A:260.) |
Genu Varum
Genu varum, or a “bowed leg” of up to 20 degrees, is normal in children until age 18 months (Fig. 432.13). Normally, it does not increase significantly after walking begins. After the child reaches the age of 24 months, genu valgum normally develops. Radiographs are indicated if genu varum is present after this age or is progressive after the age of 1 year, if it appears to be severe, or if it occurs in a high-risk group, such as obese children who walk early. Radiographic findings of benign genu varus include symmetric bowing of the tibia and femur, a normal-appearing growth plate without narrowing or step-off, and a generalized, rather than focal, outward bowing (Fig. 432.14).
Treatment involves observation to verify resolution. Objective assessment may be accomplished by measuring the distance between the femoral condyles. This method is not as accurate as are radiographs, but these measurements are a practical way of observing change in patients when the presumptive diagnosis is physiologic genu varum.
 FIGURE 432.14. Note improvement in physiologic bowing between A: age 18 months and B: 24 months without treatment. |
The differential diagnosis of physiologic genu varum includes Blount disease, rickets, posttraumatic growth-plate disturbance, enchondromatosis, achondroplasia, and other skeletal dysplasias. The ratio of physiologic bowing to Blount disease is more than 1,000:1.
Tibia Vara (Blount Disease)
Tibia vara, also known as Blount disease, is an idiopathic, probably mechanical deficiency in the medial tibial growth plate that may be unilateral or bilateral. Initially, it may present in two different age groups: infants and adolescents.
Almost always, untreated infantile tibia vara is progressive and, in addition to exhibiting outward angulation, includes flexion, internal rotation and, often, abnormal lateral knee laxity. Radiography demonstrates progressive depression of the medial metaphysis, the growth plate, and the epiphysis and, eventually, fusion of the medial metaphysis to the epiphysis in severe cases. A helpful early distinction in tibia vara is the focal nature of the change, with sharp angulation of the proximal tibial metaphysis resulting in a metaphyseal-diaphyseal angle of 11 to 16 degrees or more, measured as shown in Figure 432.15. It is a specific sign, because such localized angulation occurs in fewer than 5% of children with physiologic varus but is seen in essentially all those with Blount disease.
Brace treatment usually is used for mild but definite cases of Blount disease. Valgus rotational osteotomy of the tibia is indicated if the angulation persists beyond 3 years. Recurrence is common if treatment begins after age 4, if the epiphysis is fragmented, or if an affected child is obese. Persistent tibia vara leads to early degenerative changes.
Adolescent tibia vara has its onset in children older than age 9. It is most common in obese boys. Probably, it is caused by decreased growth of the medial tibial physis resulting from excessive medial stresses. Radiography shows medial femoral and tibial bowing. Bracing is not practical in these obese adolescents. Treatment involves osteotomy to realign the limb or lateral growth-plate closure to allow growth to “catch up” medially.
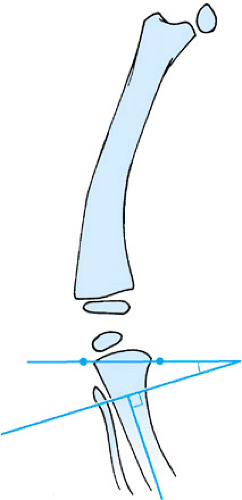 FIGURE 432.15. Metaphyseal-diaphyseal angle. The angle is formed by the line of the tibial shaft and the line between the medial and lateral beaks of the proximal tibial metaphysis. (Redrawn with permission from Levine AM. Physiologic bowing and tibia varum. J Bone Joint Surg 1982;64A:1159.) |
Genu Valgum
Genu valgum is normal in children older than age 2, reaches a mean of 12 degrees at age 3, and remains approximately constant at a mean of approximately 7 degrees in boys and 9 degrees in girls after age 8. If the angle remains greater than 15 degrees when the child reaches age 10, early growth-plate stapling or later osteotomy of the affected region may be indicated. Valgus of the proximal tibia often follows medial metaphyseal fractures, but frequently it corrects spontaneously.
Tibia
Internal Tibial Torsion
Internal tibial torsion is the most common cause of toeing-in in children between ages 1 and 3. The child with tibial torsion typically has knees that point outward while the feet point inward. Tibial torsion is determined by measuring the angle between the foot and the thigh, with the ankle and knee positioned at 90 degrees. Normally, the foot rotates externally with age (Fig. 432.16). The differential diagnosis includes metatarsus adductus, femoral anteversion, and neuromuscular disorders. To make these distinctions, the foot as well as the hip should be examined (see Fig. 432.16A–C). Tibial torsion improves naturally with growth, but this improvement often takes years. Because of our improved knowledge of the benign natural history of this condition, bracing with such devices as the Denis-Browne bar is used only rarely. Studies have shown that braces cannot apply significant rotational force to the tibia, because the corrective force is taken up in the foot, knee, and hip joints. The improvement that previously was attributed to the brace is primarily the result of normal growth patterns. Correction is a slow process and often frustrates parents. Knowledge that braces were used heavily in the past, reinforced by grandparents and friends, often drives anxious parents to visit the doctor to ensure that they are not missing a golden opportunity to avoid problems. Attendant physicians should be confident in allaying such anxiety and should advise them in some such fashion as, “Your child is toeing-in because of inward twisting of the tibia, or leg bone. This is a normal stage in resolution of the position in the womb. Some children have more toeing-in than others. Although such children occasionally may catch a foot when they run, this will improve. As the bone grows longer, it will grow straighter. It may take a few years to correct. Doctors used to use braces for this, but we found that children were getting better by themselves. You can reassure friends and relatives that the child will outgrow it.” Use of the graph shown in Figure 432.16C may prove convincing. Although very little evidence substantiates the efficacy of a brace or of any orthotic method, it has been a very widely used treatment that now is declining. Minor persistent internal torsion has not been shown to be detrimental.
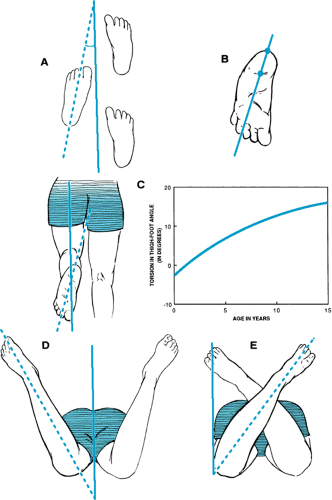 FIGURE 432.16. Assessment of torsional deformities. A: Angle of progression (the angle between the foot and the line of gait)—summation of femoral, knee, tibial, and foot relationships. B: Assessment of metatarsus adductus. Normally, the heel bisector falls between the second and third toe space. C: Thigh-foot angle and its variation with age. This is a reflection of tibial torsion. Measurement of D: internal and E: external rotation of the hip. If external rotation is less than 20 degrees, “in-toeing” may come from femoral anteversion or hip capsular contractures. (Redrawn with permission from Staheli LT, et al. Lower-extremity rotational problems in children. J Bone Joint Surg 1985;67A:41.) |
External Tibial Torsion
External tibial torsion is less common. Few data address the course of the condition, no treatment is indicated, and some spontaneous improvement can be expected.
 FIGURE 432.17. Posteromedial bow of the tibia in a 2-month-old child. This condition almost always resolves without treatment. Note the bow in the bone itself, which distinguishes it from a calcaneovalgus foot. |
Anterolateral Bowing
Mild anterolateral bowing of the tibia is common in infancy and should be observed to ensure that spontaneous straightening occurs. More severe anterolateral bowing may be associated with the radiographic finding of focal sclerotic defects in the tibia. Fractures are present or develop in affected tibias (congenital pseudarthrosis), and some affected patients may be found to have neurofibromatosis. If severe anterolateral bowing is present, but the tibia is not fractured, it should be braced for protection. If the bone is fractured, attempts to gain union by electrical stimulation, vascularized fibula grafting, and bone grafting with rod stabilization have success rates that range from 50% to 75%. Anterolateral bowing may be seen also with congenital absence of the fibula.
Posteromedial Bowing
Posteromedial bowing (Fig. 432.17) of the tibia is more benign, usually straightens by the time the child reaches age 4 years, and is not associated with fracture. Commonly, between 2 and 6 cm of shortening is seen by maturity, however. Treatment involves stretching the tight dorsiflexor muscles and the use of length equalization as indicated.
Limb-Length Inequality
Limb-length differences are screened best by palpating the heights of the iliac crests with the hips and knees straight. Any discrepancy may be confirmed with a tape measure held between the anterior superior iliac spine and the inferior edge of the medial malleolus. Most commonly, apparent differences in the lengths of the lower limbs in children are due to measurement error, because patients have difficulty in lying still and in holding hips and knees straight. In the normal population, differences of 1 cm between the two sides are not uncommon findings.
Discrepancies of up to 2 cm in adults (or a proportionately smaller amount in children) have been shown to have no ill effects on gait or joints and do not need treatment. Larger discrepancies should be confirmed with a radiographic film (scanogram) or with a CT scan. Causes of true, significant discrepancy greater than 2 cm may include hemihypertrophy, hemiatrophy, coxa vara, hip dysplasia, or growth-plate damage, to name a few. Because hemihypertrophy has been associated with Wilms tumor in some cases, these patients should be examined with abdominal ultrasonography two to three times per year until the age of 8 to 10 years. The treatment of significant limb-length inequalities may include a lift, an epiphysiodesis of the long side if growth remains, or a surgical shortening or lengthening procedure.
Foot
Metatarsus Adductus
Metatarsus adductus, or isolated idiopathic adduction of the metatarsals, is known also as metatarsus varus or C-foot. In contrast to the findings in a clubfoot, in metatarsus adductus the hindfoot is normal or angled outward slightly. The ankle joint itself has normal dorsiflexion and plantar flexion (Fig. 432.18). The probable cause of this condition is medially directed intrauterine pressure. Children with metatarsus adductus also may have an increased incidence of other molding deformities, such as congenital dislocation of the hip or torticollis. Metatarsus adductus deformity should be differentiated from skewfoot, which involves severe outward deviation of the hindfoot, the treatment of which is much more difficult. A rough measure of the degree of adduction can be obtained by determining the position of an imaginary line that would bisect the sole of the hindfoot. Normally, the line falls between the second and third toes; in patients with severe adduction, it is lateral to the fourth toe (see Fig. 432.18B).
The natural history of untreated metatarsus adductus is spontaneous correction in 85% of children, with the persistence of mild adduction in 10% and more pronounced adduction in 5%. In one longitudinal study of 2,000 feet in newborns followed until maturity, no patients had symptomatic adduction in adulthood. Those cases that will resolve spontaneously cannot be predicted, even on the basis of severity or rigidity.
The author’s preferred treatment is observation, with stretching for the first 6 to 12 months, followed by corrective casts or special shoes for the very few patients in whom the condition persists beyond this time. The casts are changed every 1 to 2 weeks until the adduction is corrected clinically. Osteotomy for very late-presenting adduction in children older than age 3 rarely is necessary.
Clubfoot
Talipes equinovarus congenita, or clubfoot, is a more complex disorder involving not only metatarsal adduction but abnormalities of the hind part of the foot, including malrotation of the calcaneus under the talus and equinus (plantar flexion) of the ankle. The incidence is 1 in 1,000, and it is more common in boys than in girls. Clubfoot may be unilateral or bilateral. Its cause is unknown, but appears to be related to a primary defect of local connective tissue or a very early insult to the leg muscles or tarsal bones.
Physical examination reveals a small foot, and the combination of deformities often results in a 90-degree rotation of the forefoot in all planes, so that the leg and foot truly resemble the shape of a club. A deep crease is present on the medial border of the foot. The deformity is not completely correctible by manual manipulation in the neonatal period, and the range of motion in all planes is limited. Radiographs are not necessary in the typical case.
Neuromuscular disorders (especially lipomeningocele, myelomeningocele, Larsen syndrome, or arthrogryposis) may produce similar deformities. Also, the genetic conditions of Mobius syndrome, diastrophic dwarfism, and Freeman-Sheldon (“whistling face”) syndrome include a deformity similar to clubfoot.
Clubfoot ranges from a mild, “postural,” and easily correctable condition to one that is severe and resistant to treatment.
A trial of cast correction is indicated in all cases, however. This treatment is most successful when started in the perinatal period, when ligamentous laxity is greatest, with the casts being changed once to twice per week. The residual tight heel cord may be corrected by an Achilles tenotomy in the office. After the feet are corrected by casts, corrective shoes with a bar between the shoes to turn them outward, are then worn for approximately 2 years. This treatment program is commonly known as “the Ponseti method.” This method of nonoperative treatment produces better long-term results: more movement in the feet and less late pain than operative treatment. It represents a change in practice from the more operative approach taken by orthopaedic surgeons even 10 years ago. Overall, casting is effective in approximately two-thirds to three-quarters of all patients. Surgery is indicated in the others, and it involves a complete release of all bony malalignments and tendon contractures; it is performed most commonly between the ages of 6 and 12 months.
A trial of cast correction is indicated in all cases, however. This treatment is most successful when started in the perinatal period, when ligamentous laxity is greatest, with the casts being changed once to twice per week. The residual tight heel cord may be corrected by an Achilles tenotomy in the office. After the feet are corrected by casts, corrective shoes with a bar between the shoes to turn them outward, are then worn for approximately 2 years. This treatment program is commonly known as “the Ponseti method.” This method of nonoperative treatment produces better long-term results: more movement in the feet and less late pain than operative treatment. It represents a change in practice from the more operative approach taken by orthopaedic surgeons even 10 years ago. Overall, casting is effective in approximately two-thirds to three-quarters of all patients. Surgery is indicated in the others, and it involves a complete release of all bony malalignments and tendon contractures; it is performed most commonly between the ages of 6 and 12 months.
 FIGURE 432.18. Comparison of clubfoot (left) and metatarsus adductus (right). A: Lateral view, showing the equinus present only in clubfoot. B: Posterior view, showing the hindfoot varus in clubfoot but not in metatarsus adductus. C: Anterior view, showing adduction in both feet, with the varus also present in clubfoot. D: Bilateral clubfeet before and E: after treatment. |
Calcaneovalgus Foot
A calcaneovalgus foot is seen commonly in newborns; it appears dramatic but is in fact benign and self-resolving. In this condition, the foot is dorsiflexed so extremely that the dorsum of the foot is pressed against the tibia (Fig. 432.19). The cause of the disorder is intrauterine molding. Actually, the alignment of the bones of the foot internally is fine and can be verified by observing the presence of an arch and by bringing the foot to a neutral position, a movement that should not require much pressure. The toes should have normal movement. This condition should be differentiated from posteromedial bowing of the tibia, which causes the foot to assume the same direction but with a more proximal apex to the deformity and a bowing in the distal tibia. The natural history is benign. The ankle and foot stretch out naturally with time, and no cast is needed. No known sequelae accompany this condition.
Flatfoot (Pes Planovalgus)
The condition called flatfoot must be divided into flexible and rigid types. The flexible type is very common in children and usually causes no symptoms. Development of the arch of the foot occurs spontaneously during the first 8 years of life in most children. The arch of the foot is restored when weight bearing is relieved. Inward-outward motion is normal. In contrast,
rigid flatfoot may be caused by tarsal coalition, a vertical talus, neuromuscular imbalance (which occasionally also may be flexible), or arthritis of the foot. These conditions should be considered in the differential diagnosis.
rigid flatfoot may be caused by tarsal coalition, a vertical talus, neuromuscular imbalance (which occasionally also may be flexible), or arthritis of the foot. These conditions should be considered in the differential diagnosis.
 FIGURE 432.19. Calcaneovalgus foot shortly after birth, displaying significant valgus and dorsiflexion. |
The cause of the usual type of flexible flatfoot is ligamentous laxity, with mild secondary bony changes. No primary muscle abnormality exists. Occasionally, a tight heel cord may contribute by pulling the foot into greater outward angulation. Treatment is not indicated in asymptomatic cases of flexible flatfoot; prospective studies have shown that no orthotic or special shoe can produce a lasting change in pediatric flatfoot. Such devices may be indicated for rigid or neuromuscular flatfoot but not in asymptomatic children who have flexible flatfoot. The heel cord should be stretched if it is tight. Rarely is surgery indicated.
The general principles that a physician should stress to parents when asked about shoes are summarized in an article by Staheli. In short, shoes are primarily for protection; “corrective shoes” have no effect on flatfoot; and shoes should be flat, flexible, porous, and high-topped to prevent them from slipping off the foot. These characteristics are available in most reasonably priced footwear found in regular shoe stores.
Tarsal Coalition
Tarsal coalition is the failure of complete separation of hindfoot bones, with persistence of a fibrous or bony bridge or coalition between two of them. This anomaly is transmitted in an autosomal dominant fashion and is present in approximately 5% of the population. Many individuals with tarsal coalition are asymptomatic. The presence of symptoms seems to be related to the degree of outward angulation that is present, which places more shear strain on the abnormal junction.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


